Arunga Simon, Kyomugasho Naome, Kwaga Teddy, Onyango John, Leck Astrid, Macleod David, Hu Victor, Burton Matthew
Ophthalmology, Mbarara University of Science and Technology, Mbarara, Uganda.
International Centre for Eye Health, Clinical Research Department, London School of Hygiene & Tropical Medicine, London, WC1E 7HT, UK.
Wellcome Open Res. 2019 Sep 24;4:141. doi: 10.12688/wellcomeopenres.15463.1. eCollection 2019.
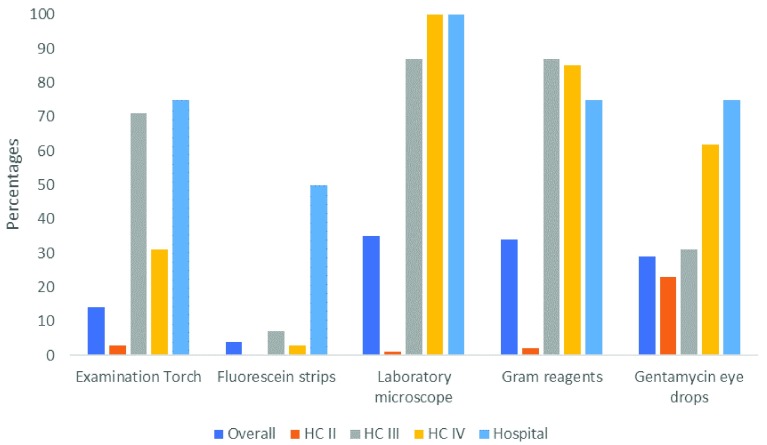
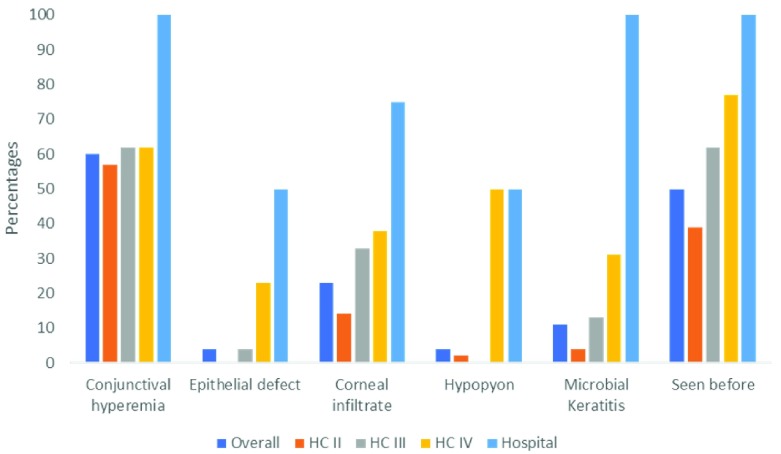
: Microbial keratitis (MK) frequently leads to sight-loss, especially when the infection is severe and/or appropriate treatment is delayed. The primary health system as an entry point plays a central role in facilitating and directing patient access to appropriate care. The purpose of this study was to describe the capacity of primary health centres in Uganda in managing MK. : We carried out a rigorous assessment of primary health centres and mid-cadre training schools in South Western Uganda. Through interviews, checklists and a picture quiz, we assessed capacity and knowledge of MK management. In addition, we interviewed the heads of all the mid-cadre training schools to determine the level of eye health training provided in their curricula. : In total, 163 health facilities and 16 training schools were enrolled. Of the health facilities, only 6% had an Ophthalmic Clinical Officer. Only 12% of the health workers could make a diagnosis of MK based on the clinical signs in the picture quiz. Although 35% of the facilities had a microscope, none reported doing corneal scraping. None of the facilities had a stock of the recommended first line treatment options for MK (ciprofloxacin and natamycin eye drops). Among the training schools, 15/16 had an eye health component in the curriculum. However, the majority (56%) of tutors had no formal expertise in eye health. In 14/16 schools, students spent an average of two weeks in an eye unit. : Knowledge among health workers and capacity of health facilities in diagnosis and management of MK was low. Training for eye health within mid-cadre training schools was inadequate. More is needed to close these gaps in training and capacity.
微生物性角膜炎(MK)常常导致视力丧失,尤其是在感染严重和/或适当治疗延迟的情况下。作为切入点的初级卫生系统在促进和引导患者获得适当护理方面发挥着核心作用。本研究的目的是描述乌干达初级卫生中心管理MK的能力。
我们对乌干达西南部的初级卫生中心和中级干部培训学校进行了严格评估。通过访谈、清单和图片测验,我们评估了MK管理的能力和知识。此外,我们采访了所有中级干部培训学校的负责人,以确定其课程中提供的眼保健培训水平。
总共纳入了163个卫生设施和16所培训学校。在这些卫生设施中,只有6%配备了眼科临床干事。在图片测验中,只有12%的卫生工作者能够根据临床体征诊断出MK。虽然35%的设施有显微镜,但没有一家报告进行角膜刮片检查。没有一家设施储备了推荐用于MK的一线治疗药物(环丙沙星和那他霉素滴眼液)。在培训学校中,16所中有15所的课程中有眼保健内容。然而,大多数(56%)教师没有眼保健方面的正规专业知识。在16所学校中的14所,学生在眼科病房平均实习两周。
卫生工作者的知识以及卫生设施在MK诊断和管理方面的能力较低。中级干部培训学校内的眼保健培训不足。需要采取更多措施来弥补培训和能力方面的这些差距。