Department of Radiology, Seoul National University-Seoul Metropolitan Government Boramae Medical Center, Seoul, Korea.
Department of Radiology, Seoul National University Hospital, Seoul, Korea.
Korean J Radiol. 2020 Mar;21(3):306-315. doi: 10.3348/kjr.2019.0060.
This study proposes a novel reference standard for hypervascular hepatocellular carcinomas (HCCs), established by cone-beam computed tomography-hepatic arteriography (CBCT-HA) and two-year imaging follow-up, and discusses its clinical implication on tumor staging and understanding the intrahepatic distant recurrence (IDR) in relation to dynamic computed tomography (CT).
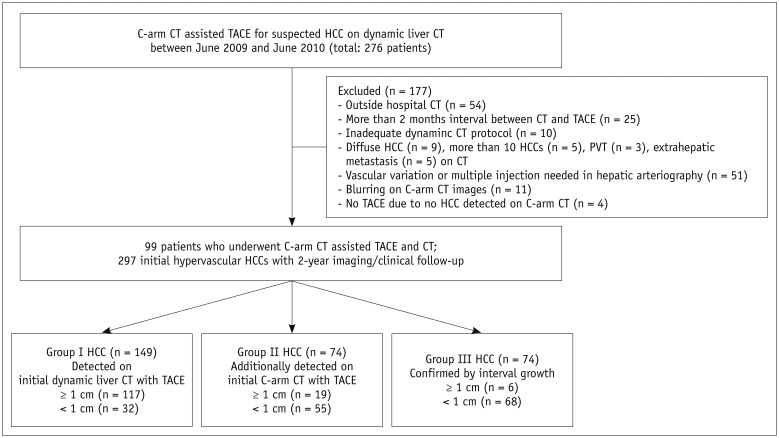
In this retrospective study, 99 patients were enrolled, who underwent CBCT-HA during initial chemoembolization for HCC suspected on CT. All patients underwent chemoembolization and regular clinical and imaging follow-up for two years. If IDR appeared on follow-up imaging, initial CBCT-HA images were reviewed to determine if a hypervascular focus pre-existed at the site of recurrence. Pre-existing hypervascular foci on CBCT-HA were regarded as HCCs in initial presentation. Initial HCCs were classified into three groups according to their mode of detection (Group I, detected on CT and CBCT-HA; Group II, additionally detected on CBCT-HA; Group III, confirmed by interval growth). We assessed the influence of CBCT-HA and two-year follow-up on initial tumor stage and calculated the proportion of IDR that pre-existed in initial CBCT-HA.
A total of 405 nodules were confirmed as HCCs, and 297 nodules initially pre-existed. Of the initial 297 HCCs, 149 (50.2%) lesions were in Group I, 74 (24.9%) lesions were in Group II, and the remaining 74 (24.9%) lesions were in Group III. After applying CBCT-HA findings, 11 patients upstaged in T stage, and 4 patients had a change in Milan criteria. Our reference standard for HCC indicated that 120 of 148 (81.1%) one-year IDR and 148 of 256 (57.8%) two-year IDR existed on initial CBCT-HA.
The proposed method enabled the confirmation of many sub-centimeter-sized, faintly vascularized HCC nodules that pre-existed initially but clinically manifested as IDR. Our reference standard for HCC helped in understanding the nature of IDR and the early development of HCC as well as the clinical impact of tumor staging and treatment decision.
本研究通过锥形束 CT 肝动脉造影(CBCT-HA)和两年影像学随访建立了一种新的富血管型肝细胞癌(HCC)参考标准,并探讨了其对肿瘤分期的临床意义以及与动态 CT 相关的肝内远处复发(IDR)的认识。
本回顾性研究纳入了 99 例在 CT 上怀疑 HCC 而行初始化疗栓塞的患者,所有患者均接受化疗栓塞和两年的定期临床和影像学随访。如果在随访影像学上出现 IDR,则对初始 CBCT-HA 图像进行复查,以确定在复发部位是否存在预先存在的富血管灶。CBCT-HA 上的预先存在的富血管灶被视为初始表现的 HCC。根据检测方式(I 组:在 CT 和 CBCT-HA 上检测到;II 组:在 CBCT-HA 上另外检测到;III 组:通过间隔生长证实)将初始 HCC 分为三组。我们评估了 CBCT-HA 和两年随访对初始肿瘤分期的影响,并计算了初始 CBCT-HA 中预先存在的 IDR 的比例。
共证实 405 个结节为 HCC,其中 297 个结节在初始时即存在。在最初的 297 个 HCC 中,149 个(50.2%)病变位于 I 组,74 个(24.9%)病变位于 II 组,其余 74 个(24.9%)病变位于 III 组。应用 CBCT-HA 结果后,11 例患者 T 分期升级,4 例患者米兰标准改变。我们的 HCC 参考标准表明,148 例 1 年 IDR 中有 120 例(81.1%)和 256 例 2 年 IDR 中有 148 例(57.8%)存在于初始 CBCT-HA 上。
该方法证实了许多直径较小、血管轻度增强的 HCC 结节最初表现为 IDR,但临床上表现为 IDR。我们的 HCC 参考标准有助于了解 IDR 的性质和 HCC 的早期发展,以及肿瘤分期和治疗决策的临床影响。