Trouillas Jacqueline, Jaffrain-Rea Marie-Lise, Vasiljevic Alexandre, Raverot Gérald, Roncaroli Federico, Villa Chiara
University of Lyon 1, University of Lyon, Lyon F-69000, France.
Faculty of Medicine Lyon-Est; Lyon, F-69372, France.
Cancers (Basel). 2020 Feb 22;12(2):514. doi: 10.3390/cancers12020514.
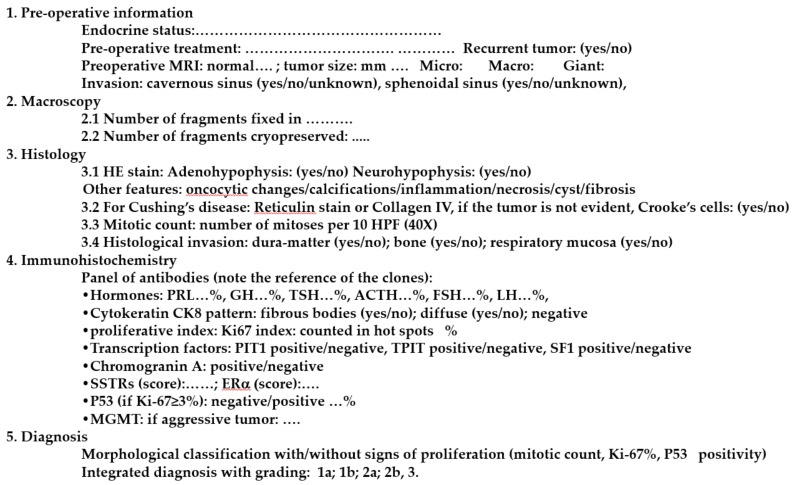
Adenohypophyseal tumors, which were recently renamed pituitary neuroendocrine tumors (PitNET), are mostly benign, but may present various behaviors: invasive, "aggressive" and malignant with metastases. They are classified into seven morphofunctional types and three lineages: lactotroph, somatotroph and thyrotroph (PIT1 lineage), corticotroph (TPIT lineage) or gonadotroph (SF1 lineage), null cell or immunonegative tumor and plurihormonal tumors. The WHO 2017 classification suggested that subtypes, such as male lactotroph, silent corticotroph and Crooke cell, sparsely granulated somatotroph, and silent plurihormonal PIT1 positive tumors, should be considered as "high risk" tumors. However, the prognostic impact of these subtypes and of each morphologic type remains controversial. In contrast, the French five-tiered classification, taking into account the invasion, the immuno-histochemical (IHC) type, and the proliferative markers (Ki-67 index, mitotic count, p53 positivity), has a prognostic value validated by statistical analysis in 4 independent cohorts. A standardized report for the diagnosis of pituitary tumors, integrating all these parameters, has been proposed by the European Pituitary Pathology Group (EPPG). In 2020, the pituitary pathologist must be considered as a member of the multidisciplinary pituitary team. The pathological diagnosis may help the clinician to adapt the post-operative management, including appropriate follow-up and early recognition and treatment of potentially aggressive forms.
腺垂体肿瘤,最近被重新命名为垂体神经内分泌肿瘤(PitNET),大多为良性,但可能呈现出各种行为:侵袭性、“侵袭性”和伴有转移的恶性行为。它们被分为七种形态功能类型和三个谱系:催乳素细胞、生长激素细胞和促甲状腺激素细胞(PIT1谱系)、促肾上腺皮质激素细胞(TPIT谱系)或促性腺激素细胞(SF1谱系)、无功能性细胞或免疫阴性肿瘤以及多激素肿瘤。世界卫生组织2017年的分类表明,诸如男性催乳素细胞、静止型促肾上腺皮质激素细胞和克鲁克细胞、稀疏颗粒型生长激素细胞以及静止型多激素PIT1阳性肿瘤等亚型应被视为“高风险”肿瘤。然而,这些亚型以及每种形态学类型的预后影响仍存在争议。相比之下,法国的五级分类法,考虑到侵袭情况、免疫组织化学(IHC)类型以及增殖标志物(Ki-67指数、有丝分裂计数、p53阳性),其预后价值已在4个独立队列中通过统计分析得到验证。欧洲垂体病理学会(EPPG)提出了一份整合所有这些参数的垂体肿瘤诊断标准化报告。在2020年,垂体病理学家必须被视为多学科垂体团队的一员。病理诊断可能有助于临床医生调整术后管理,包括适当的随访以及对潜在侵袭性形式的早期识别和治疗。