Massachusetts Veterans Epidemiology and Research Information Center (MAVERIC), Veterans Affairs Boston Healthcare System, Boston, MA, USA.
Department of Medicine, Division of Aging, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
BMC Cardiovasc Disord. 2020 Feb 26;20(1):92. doi: 10.1186/s12872-020-01384-6.
In a real-world setting, the effect of pulse rate measured at the time of diagnosis and serially during follow-up and management, on outcomes in heart failure with reduced ejection fraction (HFrEF), has not been well-studied. Furthermore, how beta-blockade use in a real-world situation modifies this relation between pulse rate and outcomes in HFrEF is not well-known. Hence, we identified a large, national, real-world cohort of HFrEF to examine the association of pulse rate and outcomes.
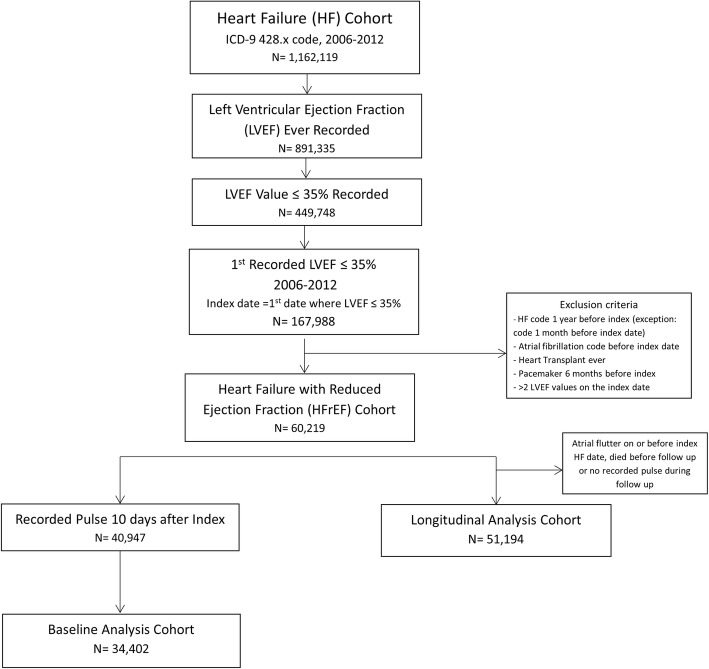
Using Veterans Affairs (VA) national electronic health records we identified incident HFrEF cases between 2006 and 2012. We examined the associations of both baseline and serially measured pulse rates, with mortality and days hospitalized per year for heart failure and for any cause, using crude and multivariable Cox proportional hazards and Poisson or negative binomial models, respectively. The exposure was examined as continuous, dichotomous, and categorical. Post-hoc analyses addressed the interaction of pulse rate and beta-blocker target dose.
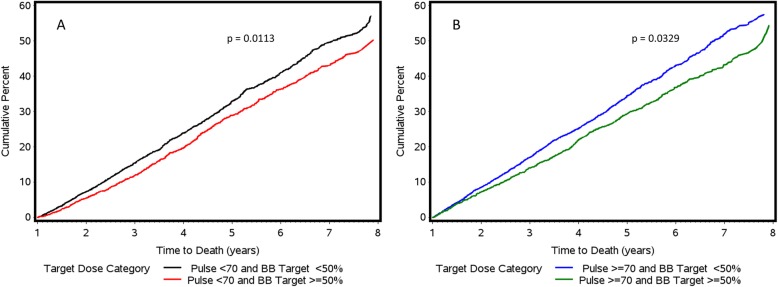
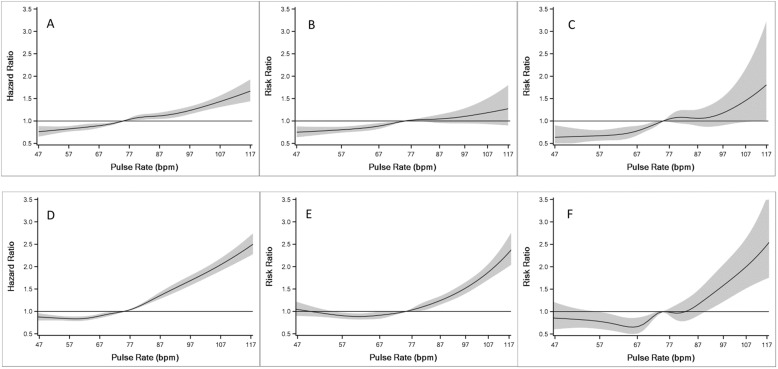
We identified 51,194 incident HFrEF cases (67 ± 12 years, 98% male, 77% white. A significant positive, near linear relationship was observed for both baseline and serially measured pulse rates with all-cause mortality, all-cause hospitalization and heart failure hospitalization after adjusting for covariates including beta-blocker use. Patients who had a pulse rate ≥ 70 bpm in the past 6 months had 36% (95% CI: 31-42%), 25% (95% CI: 19-32%), and 51% (95% CI: 33-72%) increased rates of mortality, all-cause hospitalization, and heart failure hospitalization, respectively, compared to patients with pulse rates < 70 bpm. A minority of subjects (15%) were treated with guideline directed beta blockade ≥50% of recommended target dose, among whom better outcomes were seen compared to those who did not achieve target dose in patients with pulse rates both above and below 70 beats per minute.
High pulse rate, both at the time of diagnosis and during follow-up, is strongly associated with increased risk of adverse outcomes in HFrEF patients, independent of the use of beta-blockers. In a real-world setting, the majority of HFrEF patients do not achieve target dose of beta-blockade; greater use of strategies to reduce heart rate may improve outcomes in HFrEF.
在真实环境中,脉搏率在诊断时和随访期间连续测量的效果,对射血分数降低的心力衰竭(HFrEF)的结局的影响,尚未得到很好的研究。此外,在真实情况下,β受体阻滞剂的使用如何改变 HFrEF 中脉搏率与结局之间的这种关系尚不清楚。因此,我们确定了一个大型的全国性真实世界队列,以检查脉搏率与结局之间的关系。
使用退伍军人事务部(VA)全国电子健康记录,我们在 2006 年至 2012 年间确定了 HFrEF 的新发病例。我们使用未经调整和多变量 Cox 比例风险和泊松或负二项模型,分别使用粗模型和多变量 Cox 比例风险和泊松或负二项模型,检查了基线和连续测量的脉搏率与死亡率以及每年因心力衰竭和任何原因住院的天数之间的关联。该暴露被作为连续、二分类和分类变量进行检查。事后分析解决了脉搏率和β受体阻滞剂目标剂量之间的相互作用。
我们确定了 51194 例 HFrEF 新发病例(67±12 岁,98%为男性,77%为白人)。在调整了包括β受体阻滞剂使用在内的协变量后,基线和连续测量的脉搏率与全因死亡率、全因住院和心力衰竭住院均呈显著正相关,接近线性关系。在过去 6 个月内脉搏率≥70bpm 的患者,死亡率、全因住院和心力衰竭住院的发生率分别增加 36%(95%CI:31-42%)、25%(95%CI:19-32%)和 51%(95%CI:33-72%),而脉搏率<70bpm 的患者则增加。只有少数患者(15%)接受了指南推荐的β受体阻滞剂治疗,目标剂量达到≥50%,与未达到目标剂量的患者相比,在脉搏率高于和低于 70 次/分钟的患者中,β受体阻滞剂治疗均有更好的结局。
在 HFrEF 患者中,无论是在诊断时还是在随访期间,高脉搏率与不良结局的风险增加密切相关,这与β受体阻滞剂的使用无关。在真实环境中,大多数 HFrEF 患者未能达到β受体阻滞剂的目标剂量;更多地使用降低心率的策略可能会改善 HFrEF 的结局。