Intensive Care Unit, Alice Springs Hospital, Alice Springs, NT, Australia.
Centre for Epidemiology and Biostatistics, Flinders University, Adelaide, SA, Australia.
Crit Care Resusc. 2020 Mar;22(1):35-44. doi: 10.51893/2020.1.oa4.
The apparent survival benefit of being overweight or obese in critically ill patients (the obesity paradox) remains controversial. Our aim is to report on the epidemiology and outcomes of obesity within a large heterogenous critically ill adult population.
Retrospective observational cohort study.
Intensive care units (ICUs) in Australia and New Zealand.
Critically ill patients who had both height and weight recorded between 2010 and 2018.
Hospital mortality in each of five body mass index (BMI) strata. Subgroups analysed included diagnostic category, gender, age, ventilation status and length of stay.
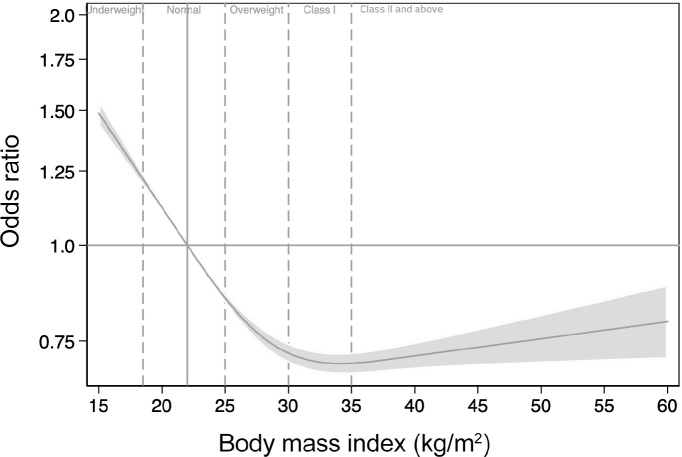
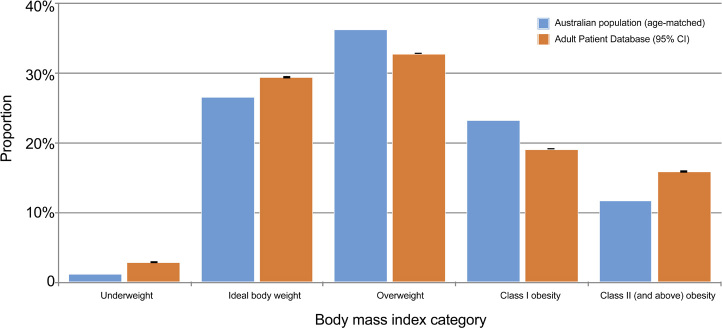
Data were available for 381 855 patients, 68% of whom were overweight or obese. Increasing level of obesity was associated with lower unadjusted hospital mortality: underweight (11.9%), normal weight (7.7%), overweight (6.4%), class I obesity (5.4%), and class II obesity (5.3%). After adjustment, mortality was lowest for patients with class I obesity (adjusted odds ratio, 0.78; 95% CI, 0.74- 0.82). Adverse outcomes with class II obesity were only seen in patients with cardiovascular and cardiac surgery ICU admission diagnoses, where mortality risk rose with progressively higher BMIs.
We describe the epidemiology of obesity within a critically ill Australian and New Zealand population and confirm that some level of obesity is associated with lower mortality, both overall and across a range of diagnostic categories and important subgroups. Further research should focus on potential confounders such as nutritional status and the appropriateness of BMI in isolation as an anthropometric measure in critically ill patients.
危重症患者超重或肥胖的生存获益明显(肥胖悖论),这一现象仍存在争议。本研究旨在报告在一个大型异质危重症成年人群中肥胖的流行病学和结局。
回顾性观察性队列研究。
澳大利亚和新西兰的重症监护病房(ICU)。
2010 年至 2018 年间身高和体重均有记录的危重症患者。
五个体重指数(BMI)分层中的每个分层的医院死亡率。分析的亚组包括诊断类别、性别、年龄、通气状态和住院时间。
共纳入 381855 例患者,其中 68%超重或肥胖。肥胖程度的增加与未调整的医院死亡率降低相关:体重不足(11.9%)、正常体重(7.7%)、超重(6.4%)、I 级肥胖(5.4%)和 II 级肥胖(5.3%)。调整后,I 级肥胖患者的死亡率最低(调整后的优势比,0.78;95%CI,0.74-0.82)。仅在心血管和心脏手术 ICU 入院诊断的患者中,II 级肥胖才与不良结局相关,且 BMI 越高,死亡率越高。
本研究描述了澳大利亚和新西兰危重症人群中肥胖的流行病学,并证实一定程度的肥胖与死亡率降低相关,无论是总体死亡率还是在一系列诊断类别和重要亚组中均如此。进一步的研究应集中于潜在的混杂因素,如营养状况以及 BMI 作为危重症患者的人体测量指标的适宜性。