University of Cologne, Dept. of Internal Medic University Hospital of Cologne, Germany.
University of Würzburg, Medical Center, Medical Clinic II, Würzburg, Germany.
Haematologica. 2021 Feb 1;106(2):543-554. doi: 10.3324/haematol.2019.223693.
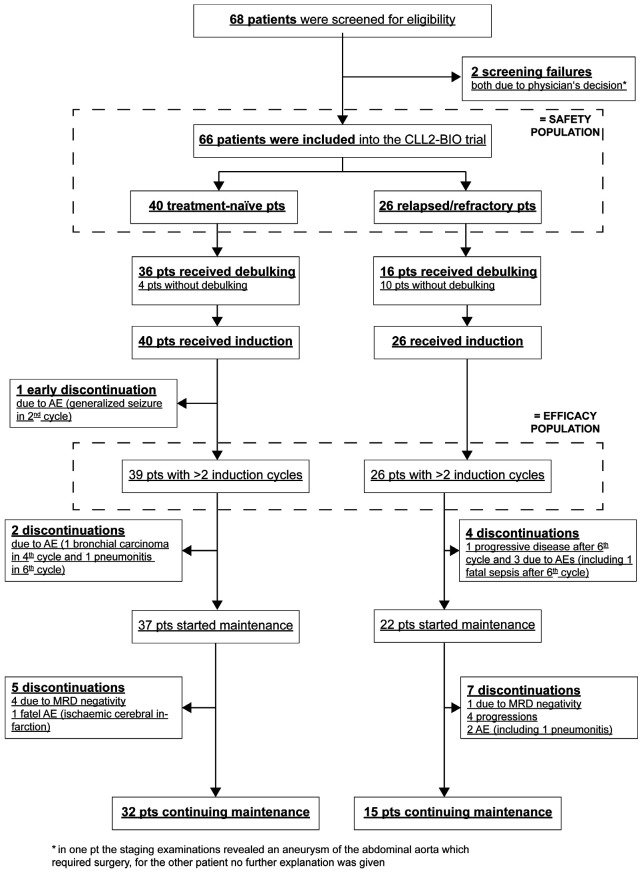
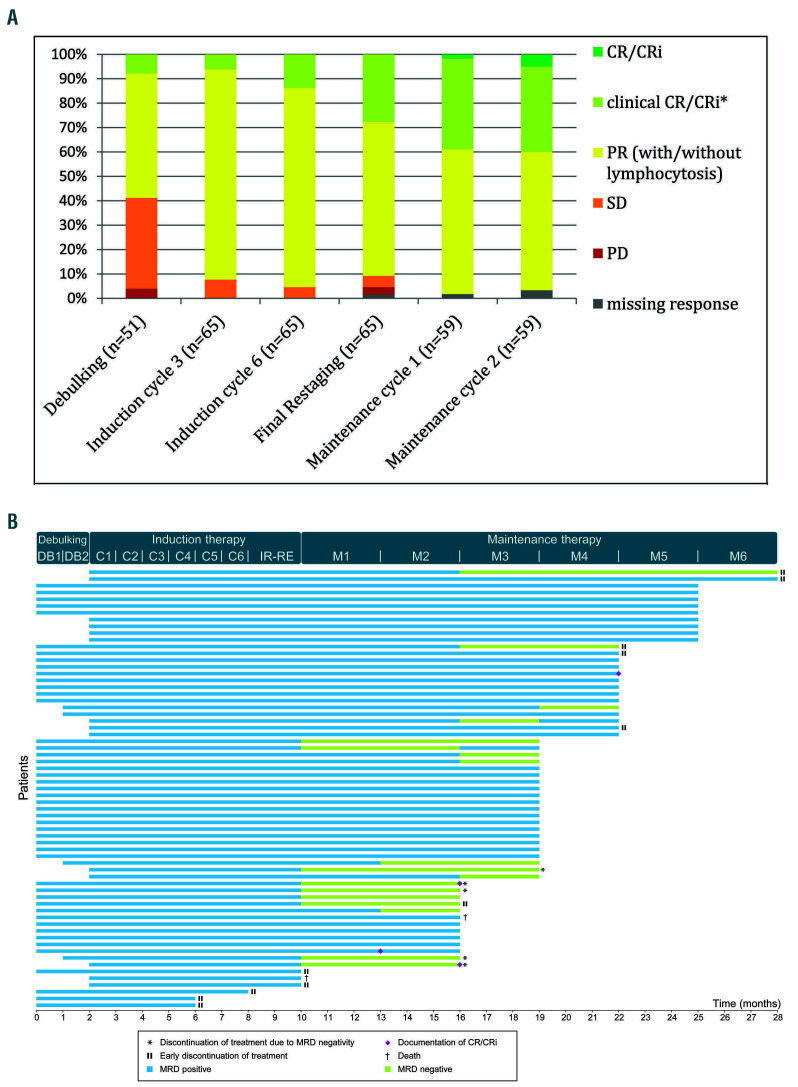
The introduction of targeted agents has revolutionized the treatment of chronic lymphocytic leukemia but only few patients achieve complete remissions and minimal residual disease negativity with ibrutinib monotherapy. This multicenter, investigator-initiated phase-II study evaluates a sequential treatment with two cycles of bendamustine debulking for patients with a higher tumor load, followed by ofatumumab and ibrutinib induction and maintenance treatment. An all-comer population, irrespective of prior treatment, physical fitness and genetic factors was included. The primary endpoint was the investigator assessed overall response rate at the end of induction treatment. Of 66 patients enrolled, one patient with early treatment discontinuation was excluded from the efficacy analysis as predefined by the protocol. Thirty-nine patients (60%) were treatment-naive and 26 patients (40%) had relapsed/refractory CLL, 21 patients (32%) had a del(17p) and/or TP53 mutation and 45 patients (69%) had an unmutated IGHV status. At the end of the induction, 60 of 65 patients (92%) responded and 9 (14%) achieved minimal residual disease negativity (<10-4) in peripheral blood. No unexpected or cumulative toxicities occurred, most common CTC °III/IV adverse events were neutropenias, anaemia, infusion-related reactions, and diarrhoea. This sequential treatment of bendamustine debulking, followed by ofatumumab and ibrutinib was well tolerated without unexpected safety signals and showed a good efficacy with an overall response rate of 92%. Ongoing maintenance treatment aims at deeper responses with minimal residual disease negativity. However, ibrutinib should still be used as a single agent outside clinical trials. Clinicaltrials.gov number: NCT02689141.
靶向药物的引入彻底改变了慢性淋巴细胞白血病的治疗方法,但仅有少数患者接受伊布替尼单药治疗可达到完全缓解和微小残留病灶阴性。本多中心、研究者发起的 II 期研究评估了两种治疗方案,对于肿瘤负荷较高的患者,先进行两个周期的苯达莫司汀减瘤治疗,然后进行奥法妥木单抗和伊布替尼诱导及维持治疗。所有患者均入组,无论其既往治疗情况、身体状况和遗传因素如何。主要终点为诱导治疗结束时研究者评估的总体缓解率。按照方案预先设定,66 例入组患者中有 1 例因早期治疗中断而被排除在疗效分析之外。39 例(60%)患者为初治,26 例(40%)为复发/难治性 CLL,21 例(32%)有 del(17p)和/或 TP53 突变,45 例(69%)IGHV 未突变。诱导治疗结束时,65 例患者中的 60 例(92%)有反应,9 例(14%)在外周血中达到微小残留病灶阴性(<10-4)。未发生意外或累积毒性,最常见的 CTC °III/IV 不良事件为中性粒细胞减少、贫血、输注相关反应和腹泻。苯达莫司汀减瘤治疗序贯奥法妥木单抗和伊布替尼治疗耐受性良好,无意外安全性信号,总缓解率为 92%,疗效较好。目前正在进行维持治疗,旨在达到更深层次的缓解,微小残留病灶阴性。然而,伊布替尼仍应在临床试验之外作为单药使用。临床试验注册编号:NCT02689141。