China Center for Health Development Studies, Peking University, Beijing, China.
RTI International, Research Triangle Park, North Carolina.
JAMA Netw Open. 2020 Feb 5;3(2):e200241. doi: 10.1001/jamanetworkopen.2020.0241.
Progress against premature death due to noncommunicable chronic disease (NCD) has stagnated. In the United States, county-level variation in NCD premature mortality has widened, which has impeded progress toward mortality reduction for the World Health Organization (WHO) 25 × 25 target.
To estimate variations in county-level NCD premature mortality, to investigate factors associated with mortality, and to present the progress toward achieving the WHO 25 × 25 target by analyzing the trends in mortality.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study focused on NCD premature mortality and its factors from 3109 counties using US mortality data for cause of death from the Centers for Disease Control and Prevention WONDER databases and county-level characteristics data from multiple databases. Data were collected from January 1, 1999, through December 31, 2017, and analyzed from April 1 through October 28, 2019.
County-level factors, including demographic composition, socioeconomic features, health care environment, and population health status.
Variations in county-level, age-adjusted NCD mortality in the US residents aged 25 to 64 years and associations between mortality and the 4 sets of county-level factors.
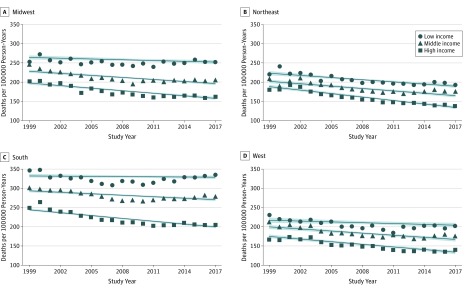
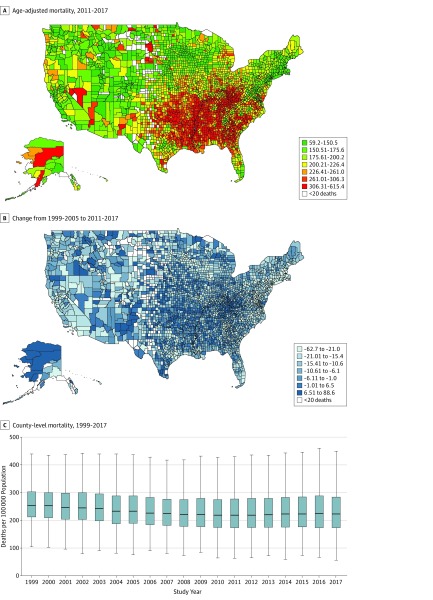
A total of 6 794 434 deaths due to NCD were recorded during the study period (50.58% women; 16.49% aged 65 years or older). Mortality decreased by 4.30 (95% CI, -4.54 to -4.08) deaths per 100 000 person-years annually from 1999 to 2010 (P < .001) and decreased annually at a rate of 0.90 (95% CI, -1.13 to -0.73) deaths per 100 000 person-years annually from 2010 to 2017 (P < .001). Mortality in the county with the highest mortality was 10.40 times as high as that in the county with the lowest mortality (615.40 vs 59.20 per 100 000 population) in 2017. Geographic inequality was decomposed by between-state and within-state differences, and within-state differences accounted for most inequality (57.10% in 2017). County-level factors were associated with 71.83% variation in NCD mortality. Association with intercounty mortality was 19.51% for demographic features, 23.34% for socioeconomic composition, 16.40% for health care environment, and 40.75% for health-status characteristics.
Given the stagnated trend of decline and increasing variations in NCD premature mortality, these findings suggest that the WHO 25 × 25 target appears to be unattainable, which may be related to broad failure by United Nations members to follow through on commitments of reducing socioeconomic inequalities. The increasing inequalities in mortality are alarming and warrant expanded multisectoral efforts to ameliorate socioeconomic disparities.
由于非传染性慢性疾病(NCD)导致的过早死亡的进展已经停滞不前。在美国,NCD 过早死亡率的县级差异已经扩大,这阻碍了世卫组织 25x25 目标的死亡率降低进展。
通过分析死亡率趋势,估计县级 NCD 过早死亡率的变化,调查与死亡率相关的因素,并展示实现世卫组织 25x25 目标的进展情况。
设计、地点和参与者:这项横断面研究使用美国疾病控制与预防中心 WONDER 数据库中的死因数据和来自多个数据库的县级特征数据,集中研究了 3109 个县的 NCD 过早死亡率及其因素。数据收集自 1999 年 1 月 1 日至 2017 年 12 月 31 日,分析时间为 2019 年 4 月 1 日至 10 月 28 日。
包括人口统计学特征、社会经济特征、医疗保健环境和人口健康状况的县级因素。
研究了美国 25 至 64 岁居民的县级年龄调整后 NCD 死亡率的变化,以及死亡率与 4 组县级因素之间的关系。
在研究期间共记录了 6794434 例 NCD 死亡(50.58%为女性;16.49%为 65 岁或以上)。死亡率从 1999 年至 2010 年每年下降 4.30(95%置信区间,-4.54 至-4.08)/100000 人年(P < 0.001),从 2010 年至 2017 年每年以 0.90(95%置信区间,-1.13 至-0.73)/100000 人年的速度下降(P < 0.001)。在 2017 年,死亡率最高的县的死亡率是死亡率最低的县的 10.40 倍(615.40 比 59.20/100000 人口)。地理不平等通过州内和州间差异进行分解,州内差异占大部分不平等(2017 年占 57.10%)。县级因素与 NCD 死亡率的 71.83%变化有关。与县间死亡率相关的因素有 19.51%为人口统计学特征,23.34%为社会经济构成,16.40%为医疗保健环境,40.75%为健康状况特征。
鉴于 NCD 过早死亡率下降趋势停滞不前且差异不断扩大,这些发现表明,世卫组织 25x25 目标似乎难以实现,这可能与联合国成员国未能履行减少社会经济不平等的承诺有关。死亡率不断增加的不平等令人震惊,需要扩大多部门努力,以改善社会经济差距。