Department of Anesthesiology, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People's Republic of China.
Department of Ultrasound, Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, 541001, People's Republic of China.
BMC Anesthesiol. 2020 Feb 28;20(1):52. doi: 10.1186/s12871-020-00969-0.
This review and meta-analysis aims to evaluate the analgesic efficacy of continuous transversus abdominis plane (TAP) block compared with epidural analgesia (EA) in adults after abdominal surgery.
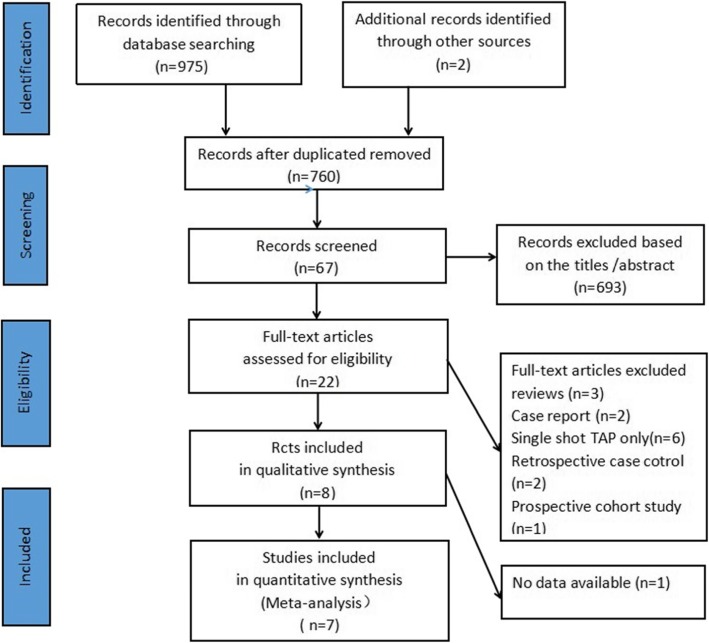
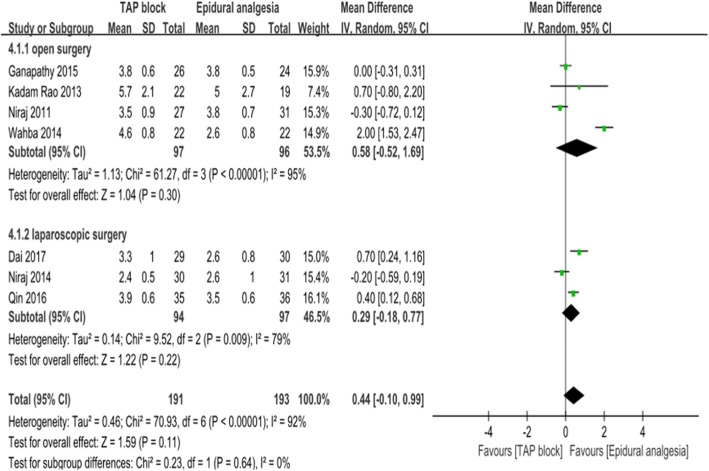
The databases PubMed, Embase and Cochrane Central Register were searched from inception to June 2019 for all available randomized controlled trials (RCTs) that evaluated the analgesic efficacy of continuous TAP block compared with EA after abdominal surgery. The weighted mean differences (WMDs) were estimates for continuous variables with a 95% confidence interval (CI) and risk ratio (RR) for dichotomous data. The pre-specified primary outcome was the dynamic pain scores 24 h postoperatively.
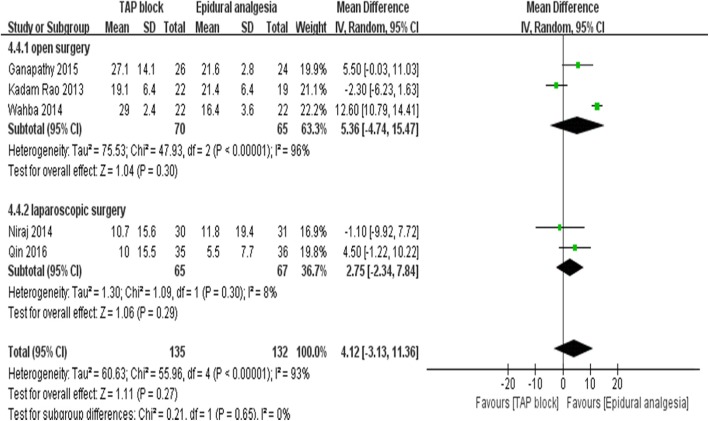
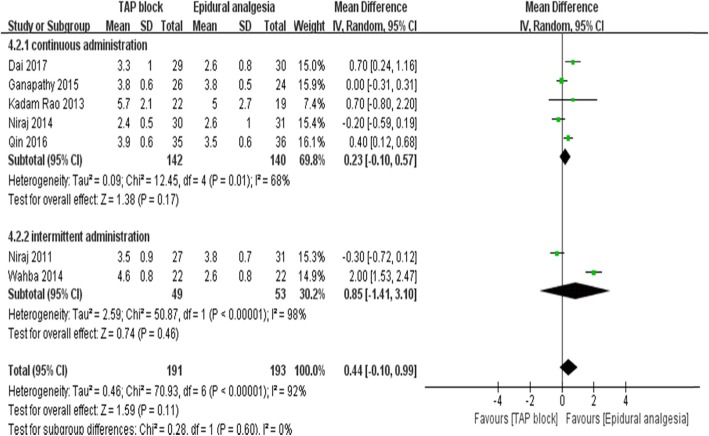
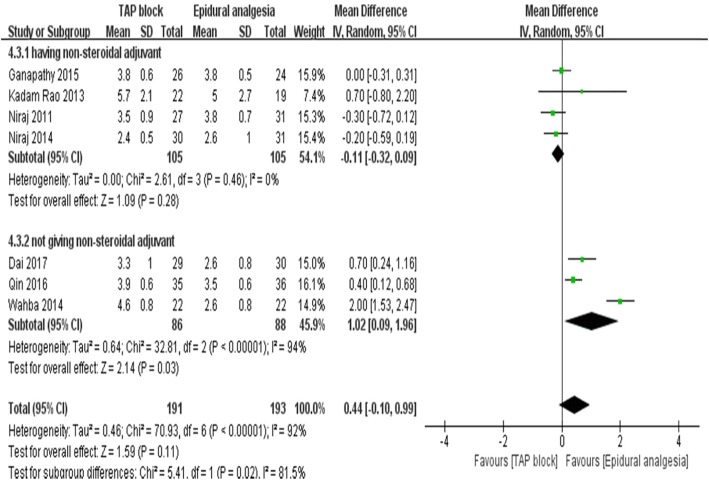
Eight trials including 453 patients (TAP block:224 patients; EA: 229 patients) ultimately met the inclusion criteria and seven trials were included in the meta-analysis. Dynamic pain scores after 24 h were equivalent between TAP block and EA groups (WMD:0.44; 95% CI: 0.1 to 0.99; I = 91%; p = 0.11). The analysis showed a significant difference between the subgroups according to regularly administering (4 trials; WMD:-0.11; 95% CI: - 0.32 to 0.09; I = 0%; p = 0.28) non-steroidal anti-inflammatory drugs (NSAIDs) or not (3 trials; WMD:1.02; 95% CI: 0.09 to 1.96; I = 94%; p = 0.03) for adjuvant analgesics postoperatively. The measured time of the urinary catheter removal in the TAP group was significantly shorter (3 trials, WMD:-18.95, 95% CI:-25.22 to - 12.71; I = 0%; p < 0.01), as was time to first ambulation postoperatively (4 trials, WMD:-6.61, 95% CI: - 13.03 to - 0.19; I = 67%; p < 0.05).
Continuous TAP block, combined with NSAIDs, can provide non-inferior dynamic analgesia efficacy compared with EA in postoperative pain management after abdominal surgery. In addition, continuous TAP block is associated with fewer postoperative side effects.
本综述和荟萃分析旨在评估腹部手术后连续腹横肌平面(TAP)阻滞与硬膜外镇痛(EA)相比的镇痛效果。
从建库至 2019 年 6 月,我们检索了 PubMed、Embase 和 Cochrane 中央注册数据库,以获取所有评估腹部手术后连续 TAP 阻滞与 EA 相比镇痛效果的随机对照试验(RCT)。连续变量的加权均数差值(WMD)采用 95%置信区间(CI)和二分类数据的风险比(RR)进行估计。主要结局是术后 24 小时的动态疼痛评分。
最终纳入 8 项 RCT,共 453 例患者(TAP 阻滞组:224 例;EA 组:229 例),7 项 RCT 纳入荟萃分析。术后 24 小时动态疼痛评分在 TAP 阻滞组和 EA 组之间无差异(WMD:0.44;95%CI:0.1 至 0.99;I=91%;p=0.11)。根据术后是否常规给予(4 项 RCT;WMD:-0.11;95%CI:-0.32 至 0.09;I=0%;p=0.28)或不给予(3 项 RCT;WMD:1.02;95%CI:0.09 至 1.96;I=94%;p=0.03)非甾体类抗炎药(NSAIDs),亚组分析显示组间存在显著差异。TAP 组尿管拔除时间明显缩短(3 项 RCT,WMD:-18.95;95%CI:-25.22 至 -12.71;I=0%;p<0.01),术后首次下床时间也明显缩短(4 项 RCT,WMD:-6.61;95%CI:-13.03 至 -0.19;I=67%;p<0.05)。
与 EA 相比,腹部手术后连续 TAP 阻滞联合 NSAIDs 可提供非劣效的术后动态镇痛效果。此外,连续 TAP 阻滞与较少的术后不良反应相关。