Department of Anesthesiology, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Lab of Anesthesia & Critical Care Medicine, Translational Neuroscience Center, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
PLoS One. 2019 Jan 8;14(1):e0209646. doi: 10.1371/journal.pone.0209646. eCollection 2019.
To evaluate the analgesic efficacy of dexamethasone added to local anesthetics in ultrasound-guided transversus abdominis plane (TAP) block for the patients after abdominal surgery.
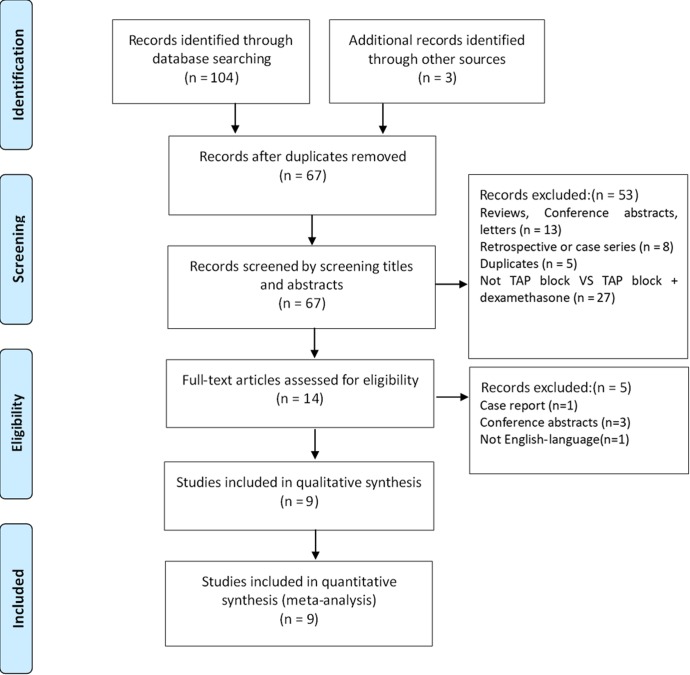
PubMed, CENTRAL, EMBASE, Web of science were searched to identify eligible randomized controlled trials (RCTs) that compared dexamethasone added to local anesthetics in ultrasound-guided TAP block with control for postoperative analgesia in adult patients undergoing abdominal surgery. Primary outcomes included postoperative pain intensity, the time to the first request for additional analgesics, and opioid consumption over 24 h after surgery. Secondary outcome was the incidence of postoperative nausea and vomiting. Analysis was performed by RevMan 5.3 software and the quality of evidence was rated using GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach.
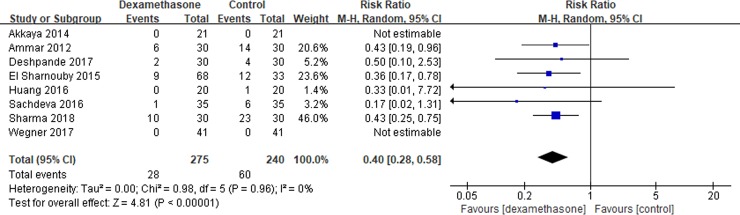
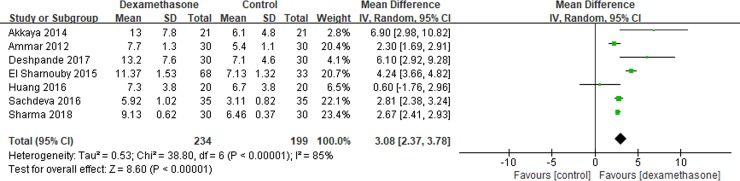
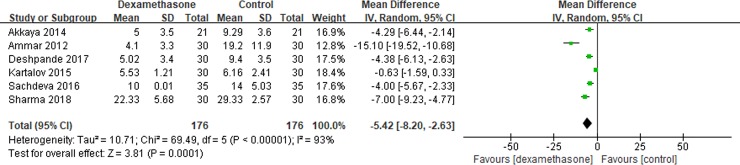
Nine RCTs involving 575 patients were included. Compared to the control, dexamethasone added to local anesthetics in ultrasound-guided TAP block significantly decreased visual analogue scale (VAS) scores at rest at 4h (mean difference [MD] = -1.01; 95% confidence intervals [CI], -1.29 to -0.73; P<0.00001; moderate quality of evidence), 6h (MD = -1.21; 95% CI, -1.74 to -0.69; P<0.00001; low quality of evidence), and 12h after surgery (MD = -0.79; 95% CI, -0.97 to -0.60; P<0.00001; moderate quality of evidence). No difference was found at 2h (MD = -0.64; 95% CI, -1.35 to 0.08; P = 0.08; low quality of evidence) and 24 h (MD = -0.41; 95% CI, -0.91 to 0.09; P = 0.11; moderate quality of evidence) in VAS scores. The time to the first request for additional analgesics was prolonged in the dexamethasone group (MD = 3.08; 95% CI, 2.37 to 3.78; P<0.00001; moderate quality of evidence). Opioid consumption over 24 h after surgery was also reduced (MD = -5.42; 95% CI, -8.20 to -2.63; P = 0.0001; low quality of evidence). Meanwhile, the incidence of postoperative nausea and vomiting was significantly decreased in the dexamethasone group (risk ratios [RR] = 0.40; 95% CI, 0.28 to 0.58; P<0.00001; high quality of evidence). No complications were reported in all the included studies.
Dexamethasone added to local anesthetics in ultrasound-guided TAP block was a safe and effective strategy for postoperative analgesia in adult patients undergoing abdominal surgery.
评估在超声引导腹横肌平面(TAP)阻滞中加入地塞米松对腹部手术后患者的镇痛效果。
检索 PubMed、CENTRAL、EMBASE、Web of science,以确定比较超声引导 TAP 阻滞中加入地塞米松与对照组用于腹部手术后成人患者术后镇痛的随机对照试验(RCT)。主要结局包括术后疼痛强度、首次要求额外镇痛药物的时间以及术后 24 小时内的阿片类药物消耗量。次要结局是术后恶心和呕吐的发生率。采用 RevMan 5.3 软件进行分析,并使用 GRADE(推荐分级的评估、制定与评价)方法评估证据质量。
纳入了 9 项 RCT,共 575 名患者。与对照组相比,超声引导 TAP 阻滞中加入地塞米松可显著降低术后 4 小时(MD=-1.01;95%CI,-1.29 至-0.73;P<0.00001;中等质量证据)、6 小时(MD=-1.21;95%CI,-1.74 至-0.69;P<0.00001;低质量证据)和 12 小时(MD=-0.79;95%CI,-0.97 至-0.60;P<0.00001;中等质量证据)的静息状态视觉模拟量表(VAS)评分。2 小时(MD=-0.64;95%CI,-1.35 至 0.08;P=0.08;低质量证据)和 24 小时(MD=-0.41;95%CI,-0.91 至 0.09;P=0.11;中等质量证据)时 VAS 评分无差异。地塞米松组首次要求额外镇痛药物的时间延长(MD=3.08;95%CI,2.37 至 3.78;P<0.00001;中等质量证据)。术后 24 小时阿片类药物消耗量也减少(MD=-5.42;95%CI,-8.20 至-2.63;P=0.0001;低质量证据)。同时,地塞米松组术后恶心和呕吐的发生率显著降低(风险比[RR]=0.40;95%CI,0.28 至 0.58;P<0.00001;高质量证据)。所有纳入研究均未报告并发症。
在超声引导 TAP 阻滞中加入地塞米松是腹部手术后成人患者安全有效的术后镇痛策略。