Technische Universität Berlin, Berlin, Germany.
Universidad Rey Juan Carlos, Madrid, Spain.
J Neuroeng Rehabil. 2020 Feb 28;17(1):36. doi: 10.1186/s12984-020-0640-7.
FES (Functional Electrical Stimulation) neuroprostheses have long been a permanent feature in the rehabilitation and gait support of people who had a stroke or have a Spinal Cord Injury (SCI). Over time the well-known foot switch triggered drop foot neuroprosthesis, was extended to a multichannel full-leg support neuroprosthesis enabling improved support and rehabilitation. However, these neuroprostheses had to be manually tuned and could not adapt to the persons' individual needs. In recent research, a learning controller was added to the drop foot neuroprosthesis, so that the full stimulation pattern during the swing phase could be adapted by measuring the joint angles of previous steps.
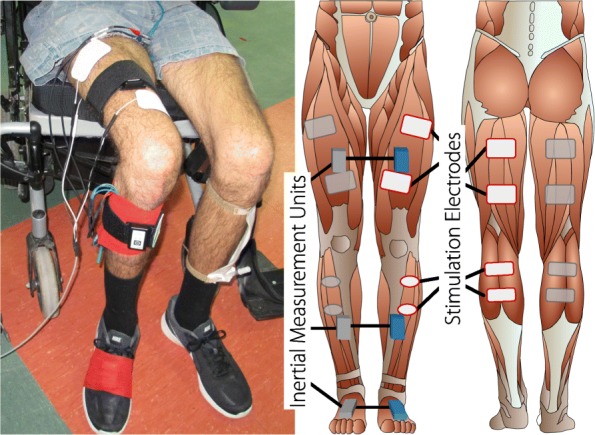
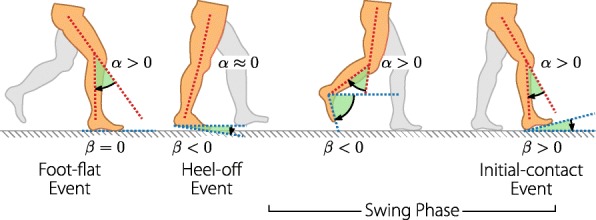
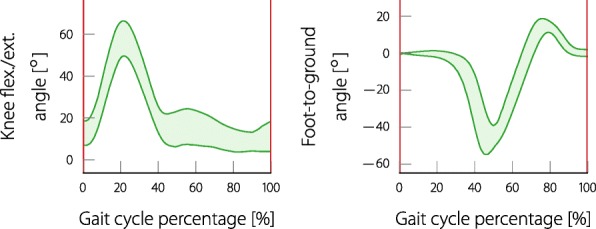
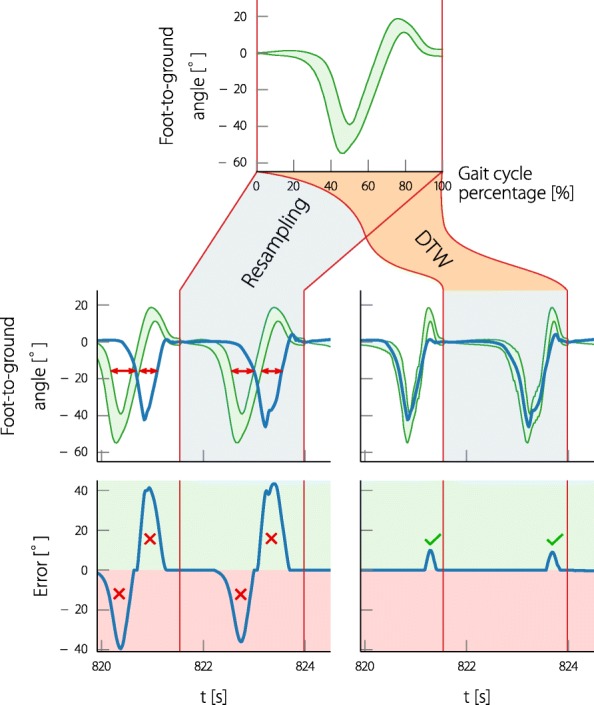
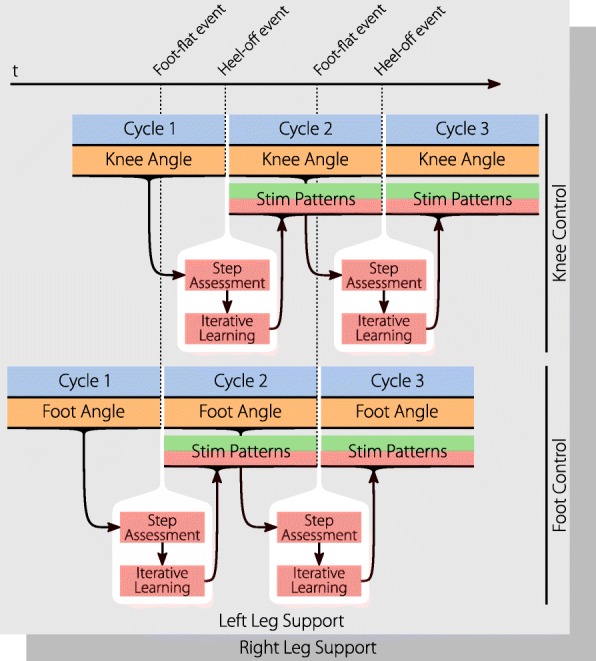
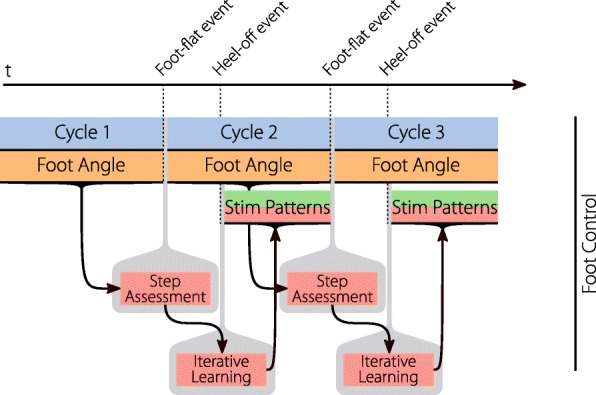
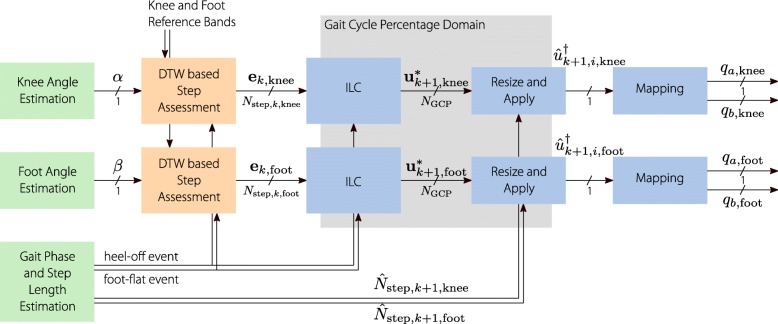
The aim of this research is to begin developing a learning full-leg supporting neuroprosthesis, which controls the antagonistic muscle pairs for knee flexion and extension, as well as for ankle joint dorsi- and plantarflexion during all gait phases. A method was established that allows a continuous assessment of knee and foot joint angles with every step. This method can warp the physiological joint angles of healthy subjects to match the individual pathological gait of the subject and thus allows a direct comparison of the two. A new kind of Iterative Learning Controller (ILC) is proposed which works independent of the step duration of the individual and uses physiological joint angle reference bands.
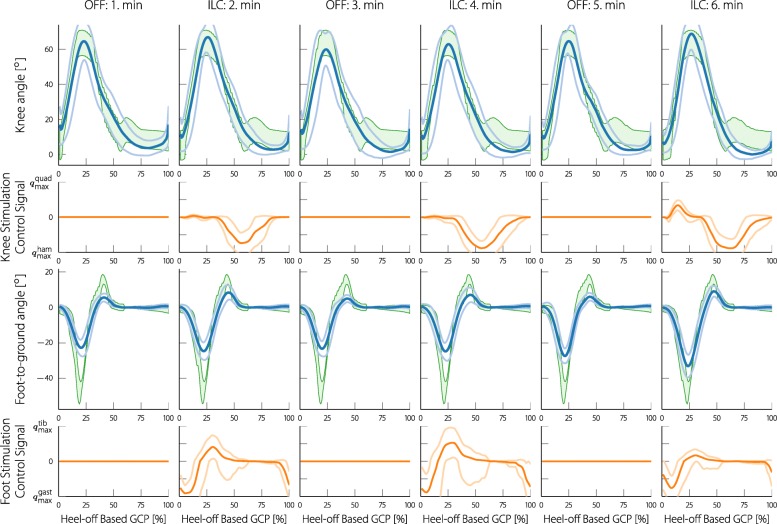
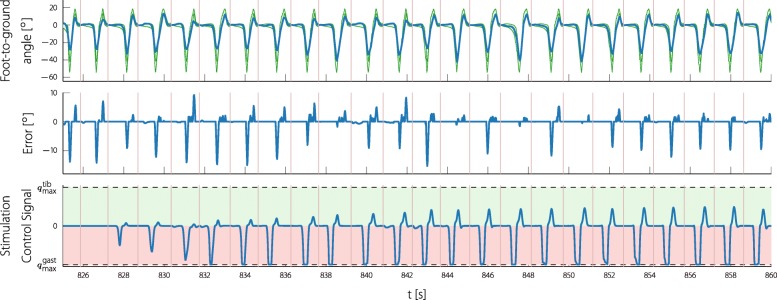
In a first test with four people with an incomplete SCI, the results showed that the proposed neuroprosthesis was able to generate individually fitted stimulation patterns for three of the participants. The other participant was more severely affected and had to be excluded due to the resulting false triggering of the gait phase detection. For two of the three remaining participants, a slight improvement in the average foot angles could be observed, for one participant slight improvements in the averaged knee angles. These improvements where in the range of 4at the times of peak dorsiflexion, peak plantarflexion, or peak knee flexion.
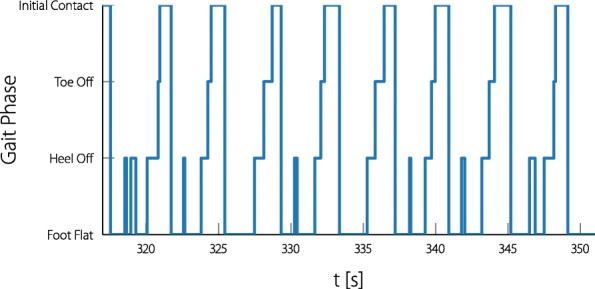
Direct adaptation to the current gait of the participants could be achieved with the proposed method. The preliminary first test with people with a SCI showed that the neuroprosthesis can generate individual stimulation patterns. The sensitivity to the knee angle reset, timing problems in participants with significant gait fluctuations, and the automatic ILC gain tuning are remaining issues that need be addressed. Subsequently, future studies should compare the improved, long-term rehabilitation effects of the here presented neuroprosthesis, with conventional multichannel FES neuroprostheses.
功能性电刺激(FES)神经假体长期以来一直是中风或脊髓损伤(SCI)患者康复和步态支持的永久性特征。随着时间的推移,众所周知的脚踏开关触发的足下垂神经假体被扩展到多通道全腿支撑神经假体,从而提供了更好的支撑和康复效果。然而,这些神经假体必须手动进行调整,并且无法适应个人的需求。在最近的研究中,在足下垂神经假体中添加了学习控制器,以便通过测量前几步的关节角度来适应摆动阶段的整个刺激模式。
本研究旨在开始开发一种学习型全腿支撑神经假体,该假体控制膝关节屈伸和踝关节背屈/跖屈的拮抗肌对,以适应所有步态阶段。建立了一种方法,允许通过每一步连续评估膝关节和踝关节的角度。该方法可以将健康受试者的生理关节角度扭曲,以匹配受试者的个体病理步态,从而可以直接比较两者。提出了一种新的迭代学习控制器(ILC),它独立于个体的步长工作,并使用生理关节角度参考带。
在对四名不完全性 SCI 患者的首次测试中,结果表明,所提出的神经假体能够为其中三名参与者生成个性化拟合的刺激模式。另一名参与者病情更严重,由于步态阶段检测的错误触发,不得不被排除在外。对于其余三名参与者中的两名,观察到平均足角度略有改善,对于一名参与者,平均膝关节角度略有改善。这些改善的范围在背屈、跖屈或膝关节屈曲峰值时为 4。
可以通过所提出的方法实现对参与者当前步态的直接适应。初步的 SCI 患者测试表明,神经假体可以生成个性化的刺激模式。仍然存在的问题包括对膝关节角度重置的敏感性、存在显著步态波动的参与者的定时问题,以及自动 ILC 增益调整。随后,未来的研究应将这里提出的神经假体与传统的多通道 FES 神经假体进行比较,以评估其长期康复效果。