Tasdogan Burcak E, Ma Michelle, Simsek Cem, Saberi Behnam, Gurakar Ahmet
Department of Gastroenterology and Hepatology, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
Department of Liver Diseases, Icahn School of Medicine at Mount Sinai, New York, USA.
Euroasian J Hepatogastroenterol. 2019 Jul-Dec;9(2):96-101. doi: 10.5005/jp-journals-10018-1301.
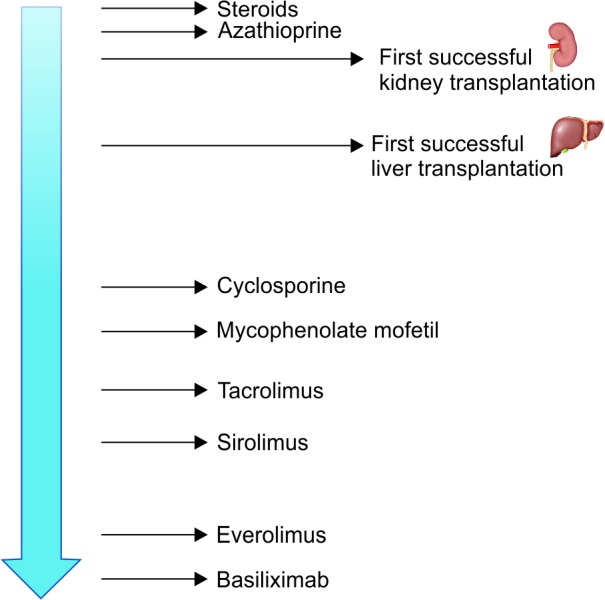
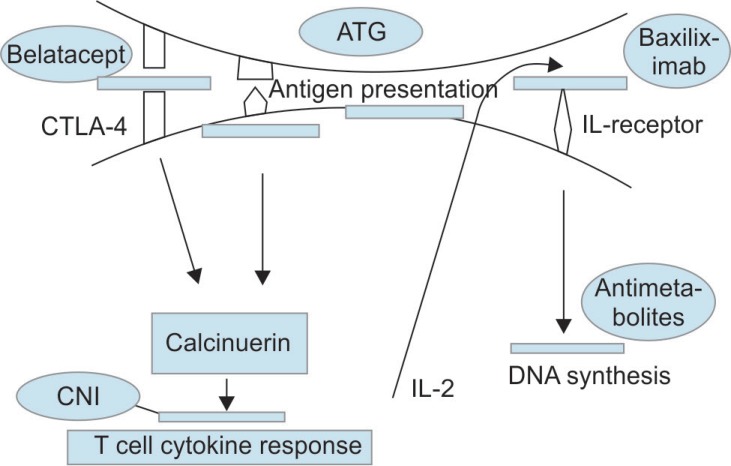
The standard therapy for decompensated end-stage chronic liver disease of any etiology and acute fulminant hepatic failure is liver transplantation (LT). Advances in immunosuppressive therapy decreased the rates of acute and chronic rejections. Thus, graft and patient survivals have significantly improved. However, long-term adverse effects of prolonged use of immunosuppressive agents such as malignancies, opportunistic infections, metabolic disorders, and other organ toxicities have now become a major concern. Consequently, alternative approaches are needed to deescalate the customary drugs and their side effects. Therapy must be individualized and additional preventive measures should be taken by patients with particular risk factors or predisposed to certain adverse effects. Current opinion favors a combination of agents with different mechanism of actions and toxicity profiles. Corticosteroids are employed in immediate and early postoperative period. Although they have a pronounced side effect profile, calcineurin inhibitors (CNIs) are still the backbone of early and late phase immunosuppressive regimens because of their proved efficacy. Antimetabolites are frequent choices for steroid and/or CNI-sparing strategies. Studies also have established a role for mammalian target of rapamycin (mTOR) inhibitors in specific groups of recipients. Biologic agents are a hot topic of interest and made their way into current strategies for induction. Agents extrapolated from other transplantation or immunologic experience are being evaluated.
Tasdogan BE, Ma M, Simsek C, . Update on Immunosuppression in Liver Transplantation. Euroasian J Hepato-Gastroenterol 2019;9(2):96-101.
对于任何病因的失代偿期终末期慢性肝病和急性暴发性肝衰竭,标准治疗方法是肝移植(LT)。免疫抑制疗法的进展降低了急性和慢性排斥反应的发生率。因此,移植物和患者的存活率有了显著提高。然而,长期使用免疫抑制剂的长期不良反应,如恶性肿瘤、机会性感染、代谢紊乱和其他器官毒性,现在已成为一个主要问题。因此,需要采取替代方法来减少常规药物及其副作用。治疗必须个体化,有特定风险因素或易发生某些不良反应的患者应采取额外的预防措施。目前的观点倾向于联合使用具有不同作用机制和毒性特征的药物。皮质类固醇用于术后即刻和早期。尽管它们有明显的副作用,但钙调神经磷酸酶抑制剂(CNIs)由于其已证实的疗效,仍然是早期和晚期免疫抑制方案的支柱。抗代谢药物是减少类固醇和/或钙调神经磷酸酶抑制剂用量策略的常用选择。研究还确立了雷帕霉素靶蛋白(mTOR)抑制剂在特定受体群体中的作用。生物制剂是一个热门话题,并已进入当前的诱导策略。从其他移植或免疫经验中推断出的药物正在进行评估。
Tasdogan BE, Ma M, Simsek C, . 肝移植免疫抑制的最新进展。《欧亚肝脏胃肠病学杂志》2019;9(2):96 - 101。