Meshram Prashant, Rhee Sung-Min, Park Joo Hyun, Oh Joo Han
Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam-si, Republic of Korea.
Shoulder & Elbow Clinic, Department of Orthopaedic Surgery, College of Medicine, Kyung Hee University, Seoul, Republic of Korea.
Orthop J Sports Med. 2020 Feb 18;8(2):2325967119899355. doi: 10.1177/2325967119899355. eCollection 2020 Feb.
Few studies have compared the clinical and radiological characteristics and outcomes in isolated subscapularis (SSC) and combined anterosuperior (AS) rotator cuff tears (RCTs). Furthermore, risk factors for retear after SSC repair and the effect of preoperative fatty degeneration require further evaluation.
To compare the functional and radiological outcomes of isolated SSC with combined AS RCTs after arthroscopic repair and to determine the risk factors for SSC retear in these 2 groups.
Cohort study; Level of evidence, 3.
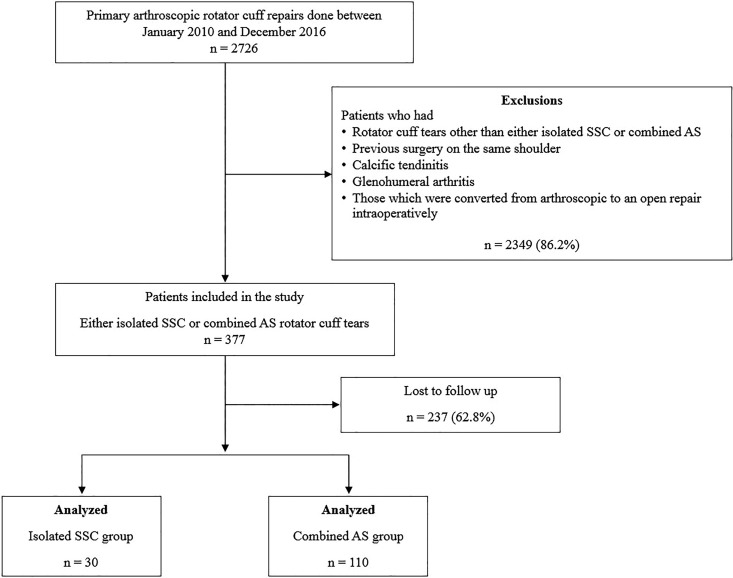
Data from 30 patients in the isolated SSC group were compared with data from 110 patients in the combined AS group. All patients underwent primary arthroscopic rotator cuff repair between 2010 and 2016. Clinical outcomes were assessed through use of the visual analog scale for pain, American Shoulder and Elbow Surgeons score, and Simple Shoulder Test at a mean follow-up of 26.7 months (range, 24-96 months). SSC tendon integrity was examined via magnetic resonance imaging, computed tomography arthrogram, or ultrasonography at least 1 year after surgery.
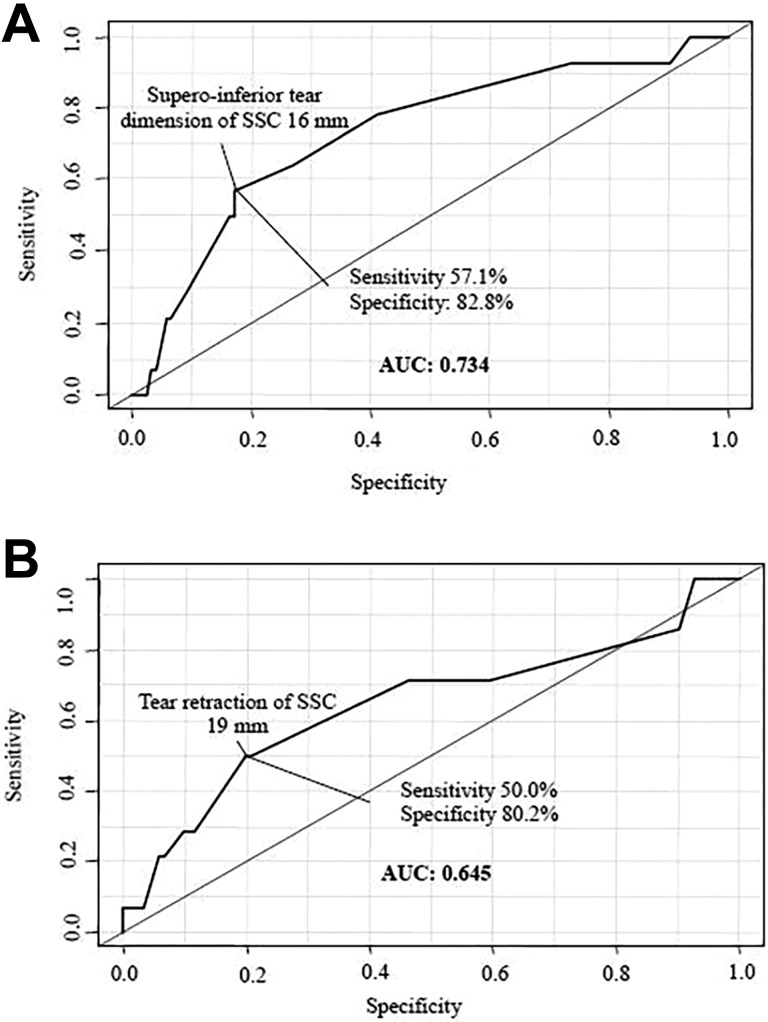
The isolated SSC group had a greater proportion of males and the patients were younger compared with the combined AS group (both < .050). The incidence of trauma was high but not significantly different between groups (56.7% vs 40.9%; = .180). Clinical outcome measures and radiological outcomes in terms of retear were not statistically different between both groups (16.7% vs 8/5%; = .337). The optimal cutoff values for the risk of SSC tendon retear in both groups were 19-mm retraction and 16-mm superoinferior dimension ( = .048). Unfavorable preoperative fatty degeneration of the SSC muscle (grades 3 and 4) was a significant risk factor for retear (odds ratio, 9.8; < .001).
Isolated SSC and combined AS RCTs were comparable except for patient age and sex; both had a high incidence of traumatic history. The current data suggest that the risk factors for retear after SSC repair in RCTs involving the SSC were tear size greater than 19 mm of retraction and unfavorable fatty degeneration (grade 3 or higher) of the SSC muscle.
很少有研究比较孤立性肩胛下肌(SSC)撕裂与合并的前上方(AS)肩袖撕裂(RCT)的临床、影像学特征及预后。此外,SSC修复术后再撕裂的危险因素以及术前脂肪变性的影响尚需进一步评估。
比较关节镜修复术后孤立性SSC撕裂与合并AS的RCT的功能和影像学预后,并确定这两组中SSC再撕裂的危险因素。
队列研究;证据等级:3级。
将孤立性SSC组30例患者的数据与合并AS组110例患者的数据进行比较。所有患者均于2010年至2016年间接受初次关节镜下肩袖修复术。在平均随访26.7个月(范围24 - 96个月)时,通过视觉模拟疼痛评分、美国肩肘外科医师协会评分和简单肩部测试评估临床预后。术后至少1年通过磁共振成像、计算机断层扫描关节造影或超声检查SSC肌腱的完整性。
与合并AS组相比,孤立性SSC组男性比例更高且患者更年轻(均P < 0.050)。创伤发生率较高,但两组间无显著差异(56.7%对40.9%;P = 0.180)。两组间在再撕裂方面的临床预后指标和影像学预后在统计学上无差异(16.7%对8.5%;P = 0.337)。两组中SSC肌腱再撕裂风险的最佳截断值分别为退缩19 mm和上下径16 mm(P = 0.048)。术前SSC肌肉脂肪变性不良(3级和4级)是再撕裂的显著危险因素(比值比,9.8;P < 0.001)。
除患者年龄和性别外,孤立性SSC撕裂与合并AS的RCT具有可比性;两者创伤史发生率均较高。目前的数据表明,在涉及SSC的RCT中,SSC修复术后再撕裂的危险因素为撕裂退缩大于19 mm以及SSC肌肉脂肪变性不良(3级或更高)。