Li Xiang, Cai Sisi, Zhong Zhaodong, Wang Hongxiang, Wang Li, You Yong, Zhang Min
Institution of Hematology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan.
Institution of Hematology, The central hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Medicine (Baltimore). 2020 Feb;99(9):e19256. doi: 10.1097/MD.0000000000019256.
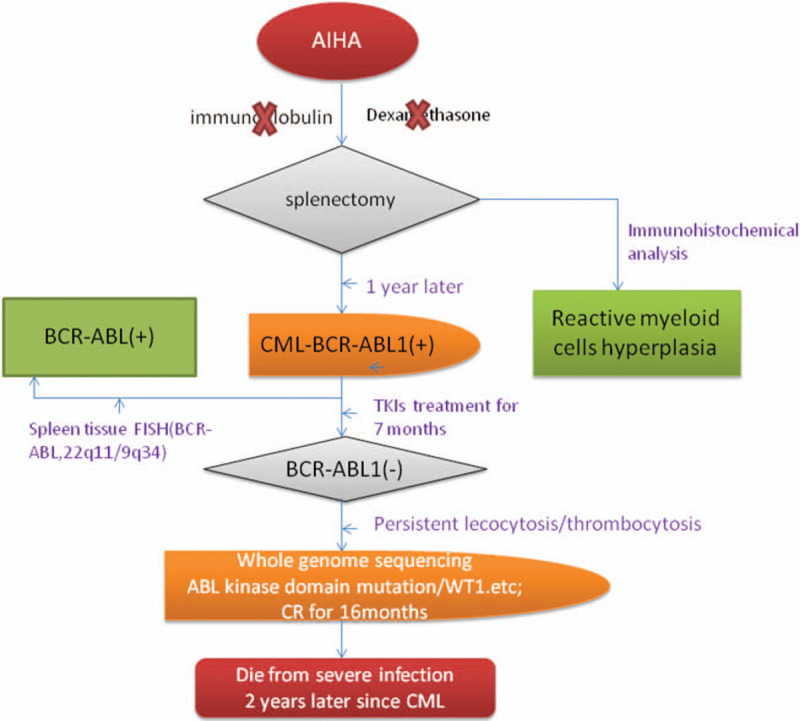
We report here the case of a patient with chronic myeloid leukemia (CML) in the chronic phase who was diagnosed 1 year after receiving a diagnosis of autoimmune hemolytic anemia (AIHA). The objective was to assess if the CML patient progressed from AIHA and explore the underlying factors of the poor outcome after the achievement of molecular complete remission (MCR).
A patient with AIHA underwent splenectomy because of poor response to immune inhibitors. The spleen biopsy showed reactive hyperplasia.
The patient was diagnosed with CML because of over-expression of the BCR-ABL (P210) gene in the bone marrow (BM), 1 year after receiving the diagnosis of AIHA.
The splenectomy was performed as the patient was unresponsive to the standard treatments consisting of immunoglobulin and dexamethasone. The removed spleen was sent for pathological examination. After she was diagnosed with CML, she received imatinib treatment.
The spleen biopsy confirmed the translocation of 22q11/9q34. No BCR-ABL kinase domain mutation was detected and there was no expression of the WT1 or EVI1 genes. After splenectomy, the number of peripheral white blood cells was consistently higher than normal during the total therapy time for CML even though she showed MCR. Two years after CML was diagnosed, the patient died from severe infection. The BM gene array analysis displayed 3 types of chromosomal abnormalities: gain (14q32.33), uniparental disomy (UPD) Xp11.22-p11.1), and UPD Xp11.1-q13.1.
AIHA may be a clinical phase of CML progression in this patient. Both splenectomy and prolonged oral tyrosine kinase inhibitors may have contributed to the high risk of infection and her subsequent death. In addition, the gain of chromosome 14q32.33 may be related to her poor outcome.
我们在此报告一名慢性期慢性髓性白血病(CML)患者的病例,该患者在被诊断为自身免疫性溶血性贫血(AIHA)1年后被确诊为CML。目的是评估该CML患者是否由AIHA进展而来,并探讨在实现分子完全缓解(MCR)后预后不良的潜在因素。
一名AIHA患者因对免疫抑制剂反应不佳而接受了脾切除术。脾活检显示反应性增生。
在被诊断为AIHA 1年后,该患者因骨髓(BM)中BCR-ABL(P210)基因过度表达而被诊断为CML。
由于患者对由免疫球蛋白和地塞米松组成的标准治疗无反应,因此进行了脾切除术。切除的脾脏送去做病理检查。在她被诊断为CML后,接受了伊马替尼治疗。
脾活检证实了22q11/9q34易位。未检测到BCR-ABL激酶结构域突变,也未检测到WT1或EVI1基因的表达。脾切除术后,尽管该患者显示出MCR,但在CML整个治疗期间外周血白细胞数量一直高于正常水平。CML确诊两年后,患者死于严重感染。BM基因阵列分析显示出3种染色体异常类型:增益(14q32.33)、单亲二体性(UPD)Xp11.22-p11.1)和UPD Xp11.1-q13.1。
AIHA可能是该患者CML进展的一个临床阶段。脾切除术和长期口服酪氨酸激酶抑制剂都可能导致感染风险增加及随后的死亡。此外,染色体14q32.33的增益可能与她的不良预后有关。