Loftus Tyler J, Tighe Patrick J, Filiberto Amanda C, Balch Jeremy, Upchurch Gilbert R, Rashidi Parisa, Bihorac Azra
Department of Surgery, University of Florida Health, Gainesville, FL, USA.
Departments of Anesthesiology, Orthopedics, and Information Systems/Operations Management, University of Florida Health, Gainesville, FL, USA.
Am J Surg. 2020 Oct;220(4):905-913. doi: 10.1016/j.amjsurg.2020.02.037. Epub 2020 Feb 26.
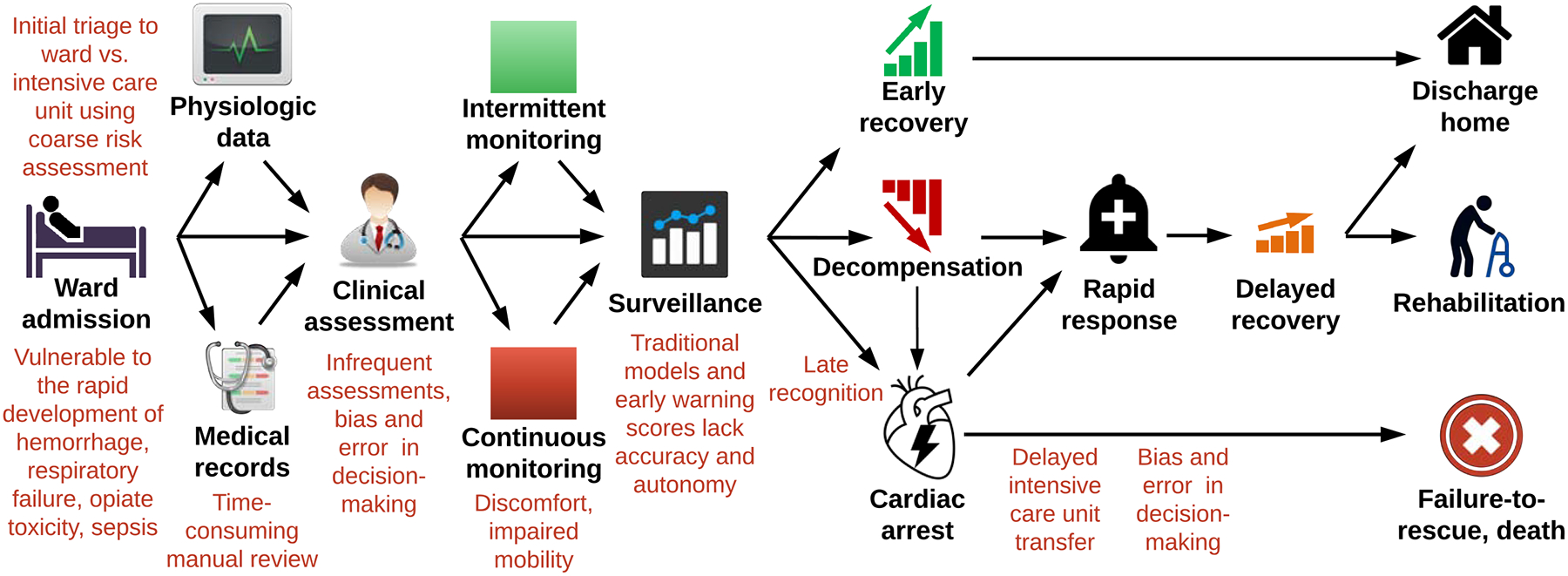
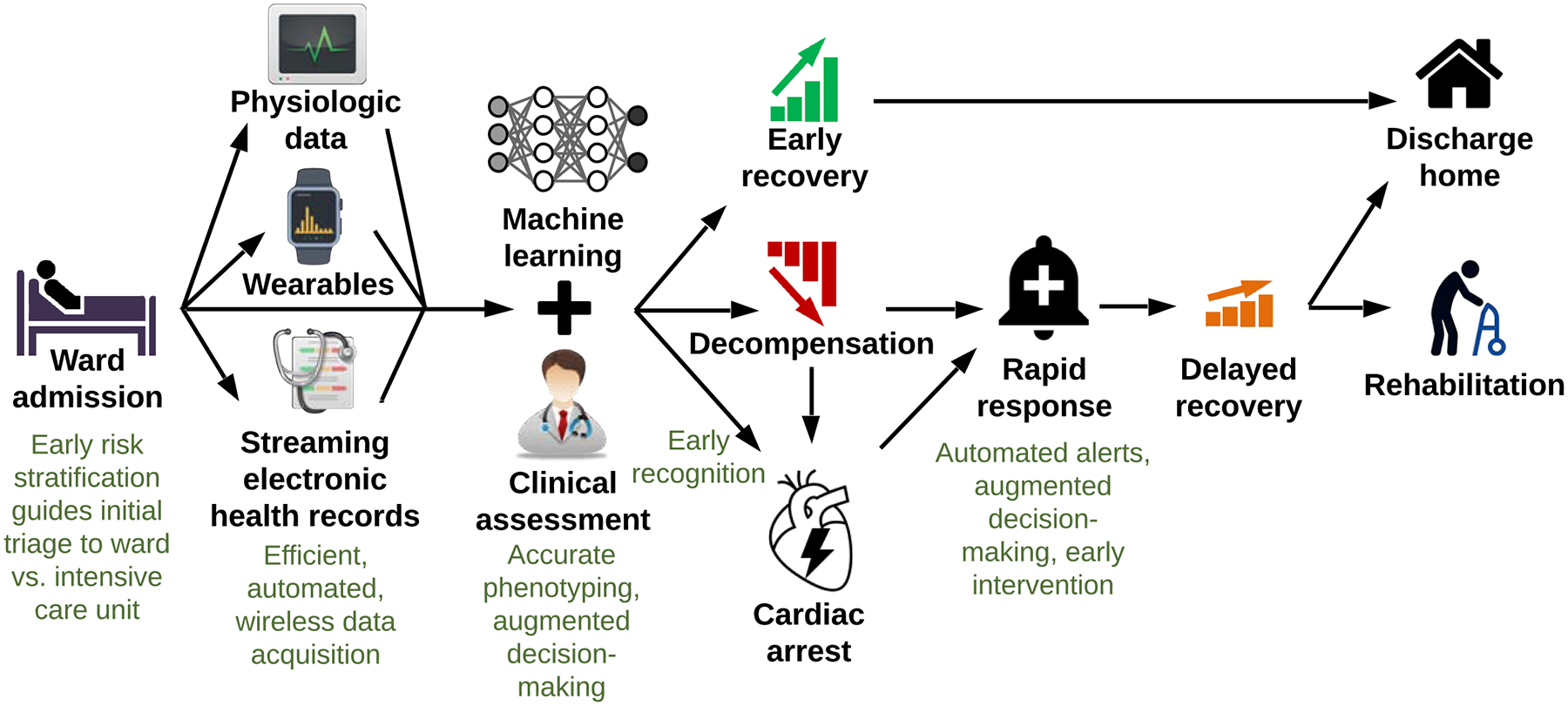
Delayed recognition of decompensation and failure-to-rescue on surgical wards are major sources of preventable harm. This review assimilates and critically evaluates available evidence and identifies opportunities to improve surgical ward safety.
Fifty-eight articles from Cochrane Library, EMBASE, and PubMed databases were included.
Only 15-20% of patients suffering ward arrest survive. In most cases, subtle signs of instability often occur prior to critical illness and arrest, and underlying pathology is reversible. Coarse risk assessments lead to under-triage of high-risk patients to wards, where surveillance for complications depends on time-consuming manual review of health records, infrequent patient assessments, prediction models that lack accuracy and autonomy, and biased, error-prone decision-making. Streaming electronic heath record data, wearable continuous monitors, and recent advances in deep learning and reinforcement learning can promote efficient and accurate risk assessments, earlier recognition of instability, and better decisions regarding diagnosis and treatment of reversible underlying pathology.
外科病房对失代偿的延迟识别和未能成功抢救是可预防伤害的主要来源。本综述汇总并批判性地评估了现有证据,并确定了改善外科病房安全性的机会。
纳入了来自考克兰图书馆、EMBASE和PubMed数据库的58篇文章。
在病房发生心脏骤停的患者中,只有15%至20%能存活。在大多数情况下,在危重病和心脏骤停之前,往往会出现细微的不稳定迹象,且潜在病理状况是可逆的。粗略的风险评估导致高危患者被分诊到病房的比例过低,在病房中,对并发症的监测依赖于耗时的健康记录人工审查、不频繁的患者评估、缺乏准确性和自主性的预测模型以及有偏差且容易出错的决策。流式电子健康记录数据、可穿戴连续监测设备以及深度学习和强化学习的最新进展可以促进高效、准确的风险评估,更早地识别不稳定情况,并就可逆性潜在病理状况的诊断和治疗做出更好的决策。