Amato Alexandre Campos Moraes, Dos Santos Ricardo Virgínio, Saucedo Dumitriu Zunino, Amato Salvador José de Toledo Arruda
Universidade Santo Amaro (UNISA), São Paulo, Brazil.
Department of Vascular Surgery, Amato-Instituto de Medicina Avançada, São Paulo, Brazil.
SAGE Open Med. 2020 Feb 22;8:2050312120909057. doi: 10.1177/2050312120909057. eCollection 2020.
Early hospital readmissions have been rising and are increasingly used for public reporting and pay-for-performance. The readmission problem is fundamentally different in surgical patients compared with medical patients. There is an opportunity to intervene preoperatively to decrease the risk of readmission postoperatively.
A predictive model of 90-day hospital readmission for patients undergoing elective carotid endarterectomy, aortofemoral bypass/aortic aneurysm repair, and femoral-distal arterial bypass was developed using data from the Healthcare Cost and Utilization Project State Inpatient Database for Florida State. The model training followed a nested resampling method with subsampling to increase execution speed and reduce overfitting. The following predictors were used: age, gender, race, median household income, primary expected payer, patient location, admission type, Elixhauser-van Walraven Comorbidity Index, Charlson comorbidity score, main surgical procedure, length of stay, disposition of the patient at discharge, period of the year, hospital volume, and surgeon volume.
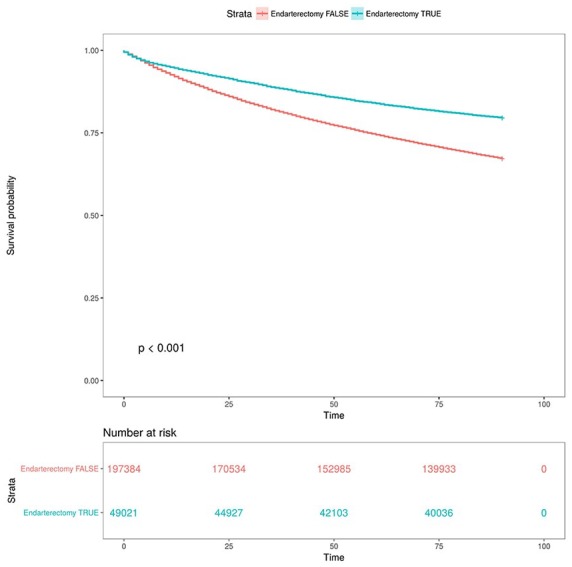
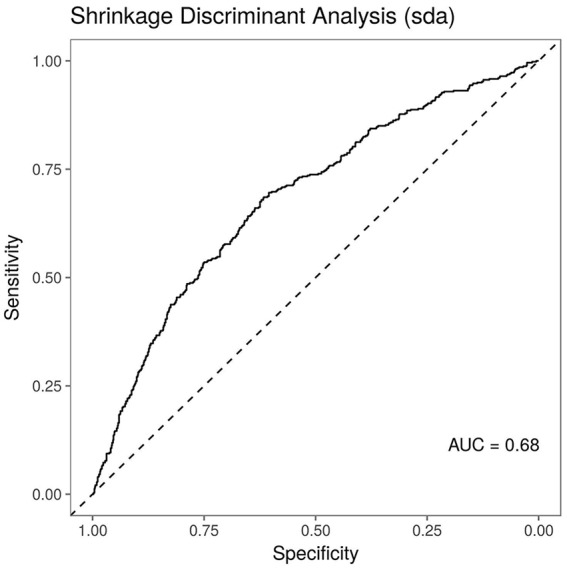
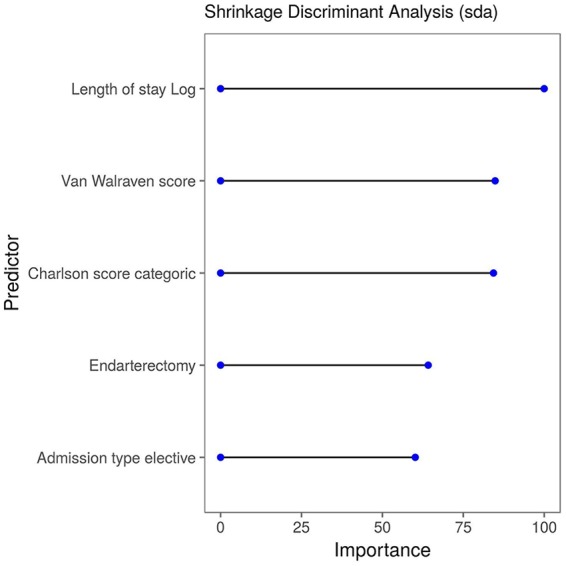
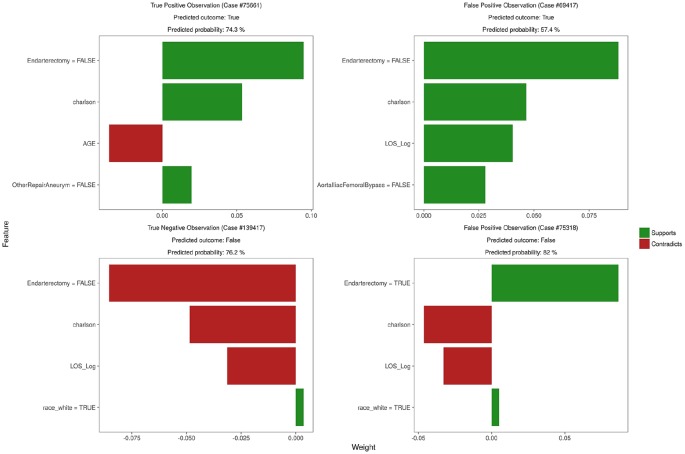
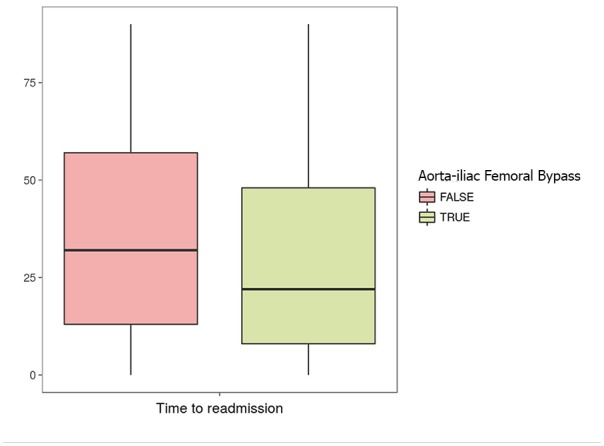
Our sample comprised data on 246,405 patients, of whom 30.3% were readmitted within 90 days. Readmitted patients were more likely to be admitted via emergency (47.2% vs 30%), included a higher percentage with a Charlson score greater than 3 (35.8% vs 18.7%), had a higher mean van Walraven score (8.32 vs 5.34), and had a higher mean length of hospital stay (6.59 vs 3.51). Endarterectomy was the most common procedure, accounting for 19.9% of all procedures. When predicting 90-day readmission, Shrinkage Discriminant Analysis was the best performing model (area under the curve = 0.68). Important variables for the best predictive model included length of stay in the hospital, comorbidity scores, endarterectomy procedure, and elective admission type. The survival analysis for the time to readmission after the surgical procedures demonstrated that the hazard ratios were higher for subjects who presented Charlson comorbidity score above three (2.29 (2.26, 2.33)), patients transferred to a short-term hospital (2.4 (2.23, 2.59)), home healthcare (1.64 (1.61, 1.68)), other type of facility (2.59 (2.54, 2.63)) or discharged against medical advice (2.06 (1.88, 2.26)), and those with greater length of stay (1.89 (1.86, 1.91)).
The model stratifies readmission risk on the basis of vascular procedure type, which suggests that attempts to decrease vascular readmission should focus on emergency procedures. Given the current focus on readmissions and increasing pressure to prevent unplanned readmissions, this score stratifies patients by readmission risk, providing an additional resource to identify and prevent unnecessary readmissions.
早期医院再入院率一直在上升,并且越来越多地用于公开报告和按绩效付费。与内科患者相比,外科患者的再入院问题有根本的不同。术前有机会进行干预以降低术后再入院风险。
利用佛罗里达州医疗成本与利用项目州住院数据库的数据,建立了接受择期颈动脉内膜切除术、主-股动脉旁路移植术/主动脉瘤修复术以及股-远端动脉旁路移植术患者90天医院再入院的预测模型。模型训练采用嵌套重采样方法及子采样,以提高执行速度并减少过拟合。使用了以下预测因素:年龄、性别、种族、家庭收入中位数、主要预期支付方、患者所在地、入院类型、埃利克斯豪泽-范瓦尔雷文合并症指数、查尔森合并症评分、主要外科手术、住院时间、出院时患者处置方式、一年中的时间段、医院手术量以及外科医生手术量。
我们的样本包含246,405例患者的数据,其中30.3%在90天内再次入院。再入院患者更可能通过急诊入院(47.2%对30%),查尔森评分大于3的患者比例更高(35.8%对18.7%),范瓦尔雷文评分均值更高(8.32对5.34),且平均住院时间更长(6.59对3.51)。内膜切除术是最常见的手术,占所有手术的19.9%。在预测90天再入院时,收缩判别分析是表现最佳的模型(曲线下面积 = 0.68)。最佳预测模型的重要变量包括住院时间、合并症评分、内膜切除术、择期入院类型。手术操作后再入院时间的生存分析表明,查尔森合并症评分高于3分的受试者(2.29(2.26,2.33))、转至短期医院的患者(2.4(2.23,2.59))、接受家庭医疗护理的患者(1.64(1.61,1.68))、转至其他类型机构的患者(2.59(2.54,2.63))或不听从医嘱出院的患者(2.06(1.88,2.26))以及住院时间更长的患者(1.89(1.86,1.91))的风险比更高。
该模型根据血管手术类型对再入院风险进行分层,这表明降低血管疾病再入院率的努力应集中在急诊手术上。鉴于当前对再入院的关注以及防止计划外再入院的压力不断增加,该评分按再入院风险对患者进行分层,为识别和预防不必要的再入院提供了额外资源。