Tulzer Andreas, Arzt Wolfgang, Prandstetter Christoph, Tulzer Gerald
Department of Pediatric Cardiology, Children's Heart Center Linz, Kepler University Hospital, Krankenhausstrasse 26-30, 4020 Linz, Austria.
Institute of Prenatal Medicine, Kepler University Hospital, Krankenhausstrasse 26-30, 4020 Linz, Austria.
Eur Heart J Case Rep. 2020 Feb 10;4(1):1-4. doi: 10.1093/ehjcr/ytaa005. eCollection 2020 Feb.
In patients with hypoplastic left heart syndrome (HLHS) premature closure or restriction of the interatrial communication causes severe cyanosis directly after birth with rapid deterioration in clinical state. An ex-utero intrapartum treatment (EXIT) procedure, extracorporal membrane oxygenation (ECMO), and emergency interventional cardiac catheterization or cardiac surgery has to be anticipated and prepared. We report the first case performing foetal atrial septum stenting in such a patient directly before birth to enable uncomplicated interatrial shunting postnatally.
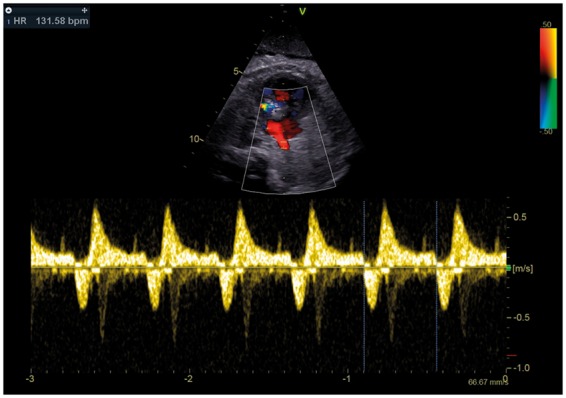
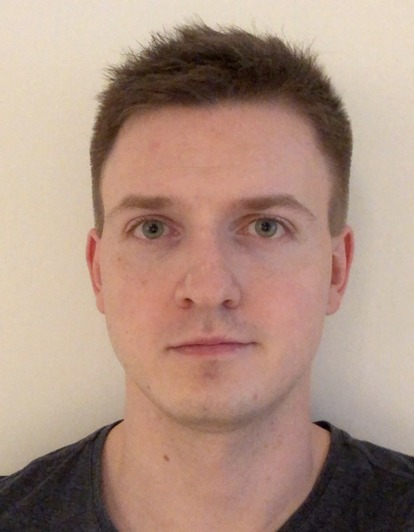
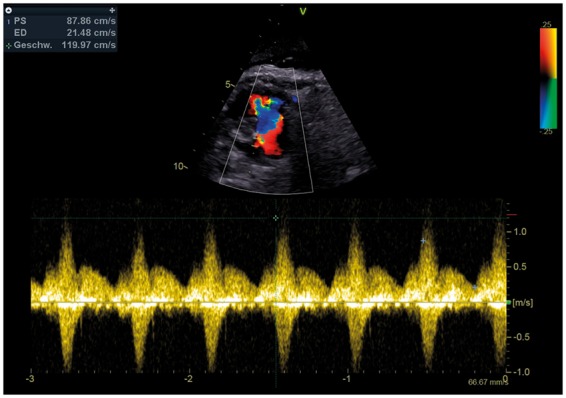
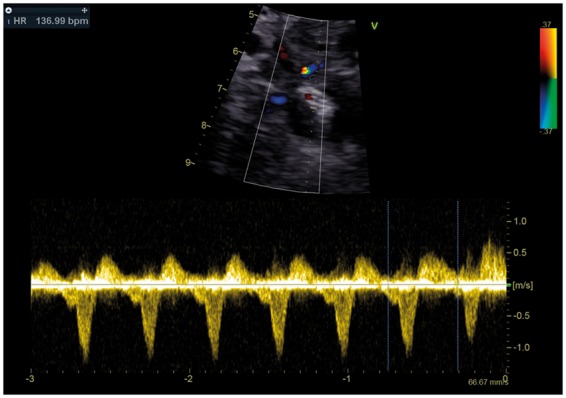
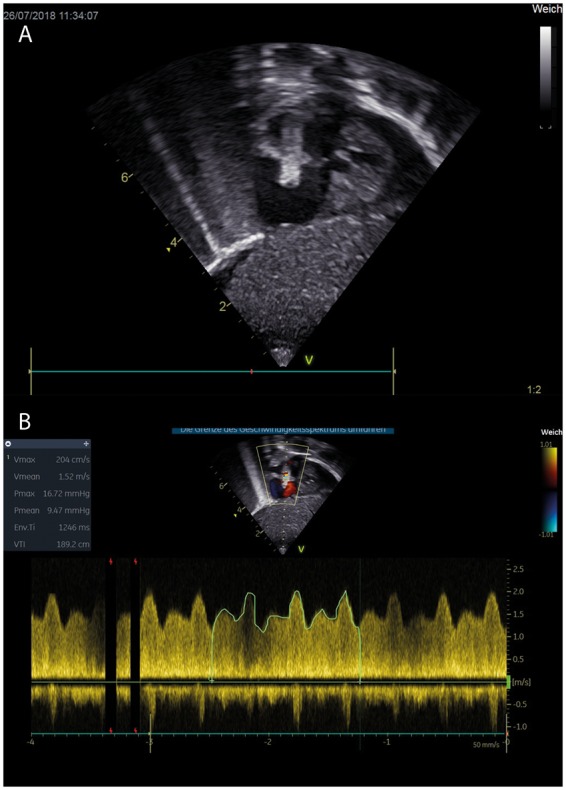
A 31-year-old pregnant woman was referred to our centre for further evaluation of the foetus due to HLHS. In the follow-up study before birth severe restriction of the foramen ovale with increased retrograde flow in the pulmonary veins [0.33 ratio antegrade/retrograde time velocity integral (TVI)] was detected. After careful consideration foetal atrial septum stenting was performed at 38 + 3 weeks of gestation. At 39 + 2 weeks of gestation the baby was born by caesarean section followed by an uncomplicated postnatal adaption. On the 7th day of life a Norwood procedure was performed and the baby was discharged on the 63rd postoperative day.
Evaluation of the interatrial communication in foetuses with HLHS should be done carefully just before birth. In the case of severe restriction or closure of the foramen ovale atrial septum stenting just before birth can be considered as an alternative treatment to an EXIT procedure, ECMO, or emergency atrioseptectomy on bypass. However, a very experienced team of paediatric cardiologists and perinatologists with expertise in foetal cardiac interventions is needed to perform this technical difficult procedure.
在左心发育不全综合征(HLHS)患者中,房间隔过早闭合或受限会在出生后直接导致严重的紫绀,并使临床状态迅速恶化。必须提前预计并准备好宫外产时治疗(EXIT)程序、体外膜肺氧合(ECMO)以及紧急介入性心导管插入术或心脏手术。我们报告了首例在出生前直接对这类患者进行胎儿房间隔支架置入术的病例,以便出生后能实现无并发症的心房间分流术治疗。
一名31岁的孕妇因HLHS被转诊至我们中心对胎儿进行进一步评估。在出生前的随访研究中,检测到卵圆孔严重受限,肺静脉逆行血流增加[顺行/逆行时间速度积分(TVI)比值为0.33]。经过仔细考虑,在妊娠38 + 3周时进行了胎儿房间隔支架置入术。在妊娠39 + 2周时,婴儿通过剖宫产出生,随后出生后适应过程顺利。出生后第7天进行了诺伍德手术,术后第63天婴儿出院。
对于患有HLHS的胎儿,应在即将出生前仔细评估心房间交通情况(即卵圆孔情况)。在卵圆孔严重受限或闭合的情况下,出生前进行房间隔支架置入术可被视为EXIT程序、ECMO或紧急体外循环下房间隔切除术的替代治疗方法。然而(在出生前进行胎儿房间隔支架置入术),需要一个由非常有经验的小儿心脏病专家和围产医学专家组成的团队(他们要有胎儿心脏介入方面的专业知识)来实施这种技术难度较大(即对操作团队要求高) 的手术。