Departments of Pathology, Loyola University Medical Center, Maywood, IL, USA.
Departments of Pharmacology, Loyola University Medical Center, Maywood, IL, USA.
Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620902849. doi: 10.1177/1076029620902849.
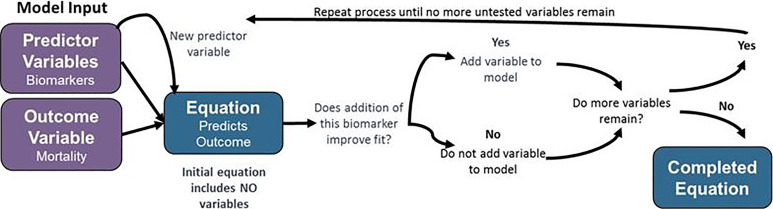
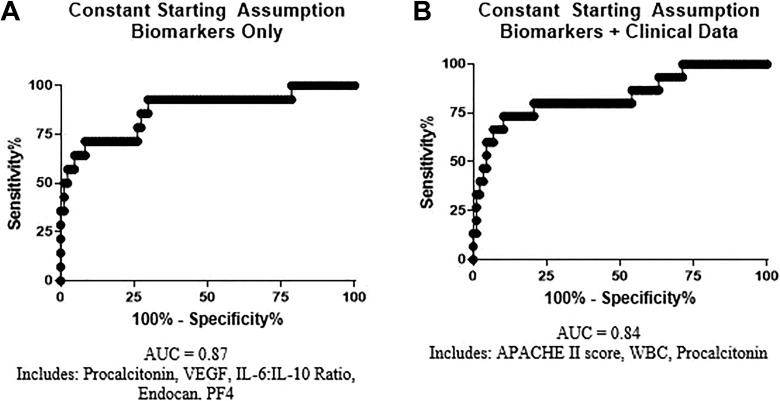
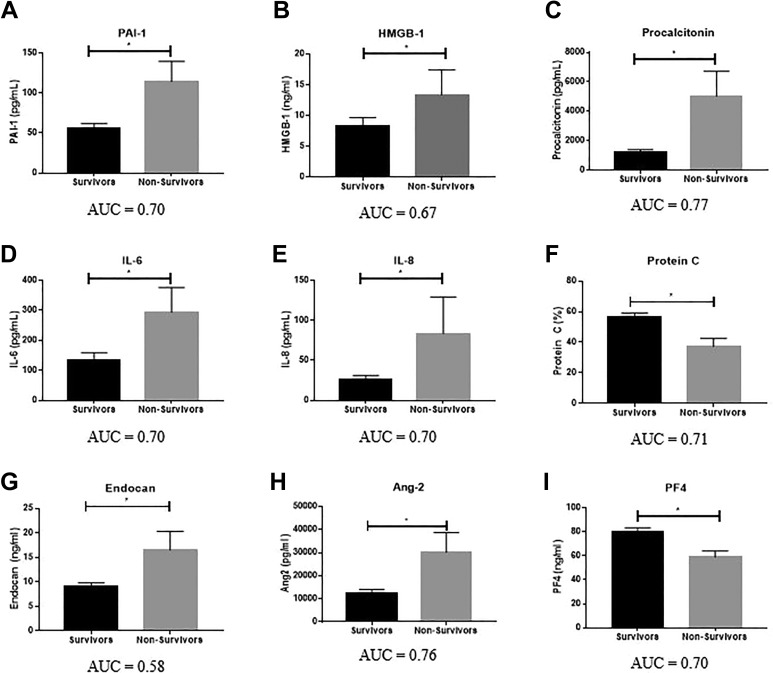
Sepsis is a systemic response to infection with a high rate of mortality and complex pathophysiology involving inflammation, infection response, hemostasis, endothelium, and platelets. The purpose of this study was to develop an equation incorporating biomarker levels at intensive care unit (ICU) admission to predict mortality in patients with sepsis, based on the hypothesis that a combination of biomarkers representative of multiple physiological systems would provide improved predictive value. Plasma samples and clinical data were collected from 103 adult patients with sepsis at the time of ICU admission. Biomarker levels were measured using commercially available methods. A 28-day mortality was used as the primary end point. Stepwise linear regression modeling was performed to generate a predictive equation for mortality. Differences in biomarker levels between survivors were quantified using the Mann-Whitney test and the area under the receiver operating curve (AUC) was used to describe predictive ability. Significant differences ( < .05) were observed between survivors and nonsurvivors for plasminogen activator inhibitor 1 (AUC = 0.70), procalcitonin (AUC = 0.77), high mobility group box 1 (AUC = 0.67), interleukin (IL) 6 (AUC = 0.70), IL-8 (AUC = 0.70), protein C (AUC = 0.71), angiopoietin-2 (AUC = 0.76), endocan (AUC = 0.58), and platelet factor 4 (AUC = 0.70). A predictive equation for mortality was generated using stepwise linear regression modeling, which incorporated procalcitonin, vascular endothelial growth factor, the IL-6:IL-10 ratio, endocan, and platelet factor 4, and demonstrated a better predictive value for patient outcome than any individual biomarker (AUC = 0.87). The use of mathematical modeling resulted in the development of a predictive equation for sepsis-associated mortality with performance than any individual biomarker or clinical scoring system which incorporated biomarkers representative of multiple systems.
脓毒症是一种全身性的感染反应,其死亡率高,病理生理学复杂,涉及炎症、感染反应、止血、内皮细胞和血小板。本研究的目的是开发一种包含重症监护病房(ICU)入院时生物标志物水平的方程,以预测脓毒症患者的死亡率,其假设是,代表多个生理系统的生物标志物组合将提供更高的预测价值。在 ICU 入院时,从 103 名成年脓毒症患者中采集血浆样本和临床数据。使用商业上可用的方法测量生物标志物水平。28 天死亡率用作主要终点。进行逐步线性回归建模,生成死亡率预测方程。使用 Mann-Whitney 检验量化幸存者和非幸存者之间的生物标志物水平差异,并使用接收者操作曲线(AUC)下的面积来描述预测能力。在幸存者和非幸存者之间观察到纤溶酶原激活物抑制剂 1(AUC = 0.70)、降钙素原(AUC = 0.77)、高迁移率族蛋白 1(AUC = 0.67)、白细胞介素 6(AUC = 0.70)、白细胞介素 8(AUC = 0.70)、蛋白 C(AUC = 0.71)、血管生成素-2(AUC = 0.76)、内皮素(AUC = 0.58)和血小板因子 4(AUC = 0.70)之间存在显著差异(<0.05)。使用逐步线性回归建模生成死亡率预测方程,该方程包含降钙素原、血管内皮生长因子、白细胞介素 6:白细胞介素 10 比值、内皮素和血小板因子 4,并且比任何单个生物标志物(AUC = 0.87)更能预测患者预后。使用数学建模的方法,开发了一种预测脓毒症相关死亡率的方程,其性能优于任何单个生物标志物或临床评分系统,该系统包含代表多个系统的生物标志物。