Carlson School of Management, University of Minnesota, Minneapolis, MN, United States.
Max Institute of Healthcare Management, Indian School of Business, Hyderabad, India.
JMIR Mhealth Uhealth. 2020 Mar 3;8(3):e15998. doi: 10.2196/15998.
Many public health programs and interventions across the world increasingly rely on using information and communications technology (ICT) tools to train and sensitize health professionals. However, the effects of such programs on provider knowledge, practice, and patient health outcomes have been inconsistent. One of the reasons for the varied effectiveness of these programs is the low and varying levels of provider engagement, which, in turn, could be because of the form and mode of content used. Tailoring instructional content could improve engagement, but it is expensive and logistically demanding to do so with traditional training.
This study aimed to discover preferences among providers on the form (articles or videos), mode (featuring peers or experts), and length (short or long) of the instructional content; to quantify the extent to which differences in these preferences can explain variation in provider engagement with ICT-based training interventions; and to compare the power of content preferences to explain provider engagement against that of demographic variables.
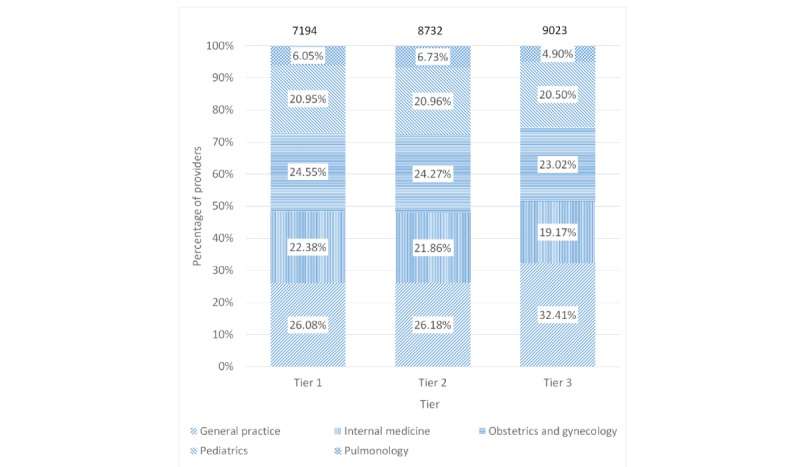
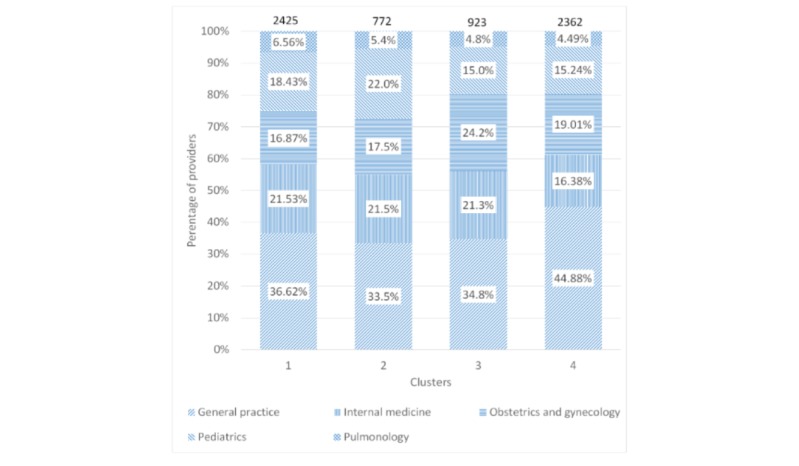
We used data from a mobile phone-based intervention focused on improving tuberculosis diagnostic practices among 24,949 private providers from 5 specialties and 1734 cities over 1 year. Engagement time was used as the primary outcome to assess provider engagement. K-means clustering was used to segment providers based on the proportion of engagement time spent on content formats, modes, and lengths to discover their content preferences. The identified clusters were used to predict engagement time using a linear regression model. Subsequently, we compared the accuracy of the cluster-based prediction model with one based on demographic variables of providers (eg, specialty and geographic location).
The average engagement time across all providers was 7.5 min (median 0, IQR 0-1.58). A total of 69.75% (17,401/24,949) of providers did not consume any content. The average engagement time for providers with nonzero engagement time was 24.8 min (median 4.9, IQR 2.2-10.1). We identified 4 clusters of providers with distinct preferences for form, mode, and length of content. These clusters explained a substantially higher proportion of the variation in engagement time compared with demographic variables (32.9% vs 1.0%) and yielded a more accurate prediction for the engagement time (root mean square error: 4.29 vs 5.21 and mean absolute error: 3.30 vs 4.26).
Providers participating in a mobile phone-based digital campaign have inherent preferences for instructional content. Targeting providers based on individual content preferences could result in higher provider engagement as compared to targeting providers based on demographic variables.

世界上许多公共卫生计划和干预措施越来越依赖于使用信息和通信技术 (ICT) 工具来培训和提高卫生专业人员的敏感性。 然而,这些计划对提供者知识、实践和患者健康结果的影响并不一致。 这些计划效果不同的原因之一是提供者参与度低且不同,而这反过来又可能是由于所使用的内容形式和模式造成的。 定制教学内容可以提高参与度,但用传统培训方法来做到这一点既昂贵又耗费精力。
本研究旨在发现提供者对教学内容形式(文章或视频)、模式(以同行还是专家为特色)和长度(短或长)的偏好; 量化这些偏好差异在多大程度上可以解释提供者对基于 ICT 的培训干预措施的参与程度的差异; 并比较内容偏好解释提供者参与度的能力与人口统计学变量的能力。
我们使用了一项基于手机的干预措施的数据,该干预措施专注于在 1 年内提高 5 个专业和 1734 个城市的 24949 名私人提供者的肺结核诊断实践。 将参与时间用作评估提供者参与度的主要结果。 使用 K-均值聚类根据内容格式、模式和长度的参与时间比例对提供者进行细分,以发现他们的内容偏好。 使用线性回归模型,根据聚类识别的偏好来预测参与时间。 随后,我们比较了基于提供者人口统计学变量(例如专业和地理位置)的预测模型与基于聚类的预测模型的准确性。
所有提供者的平均参与时间为 7.5 分钟(中位数 0,IQR 0-1.58)。 共有 69.75%(17401/24949)的提供者没有消费任何内容。 有非零参与时间的提供者的平均参与时间为 24.8 分钟(中位数 4.9,IQR 2.2-10.1)。 我们确定了 4 组具有不同内容形式、模式和长度偏好的提供者。 与人口统计学变量(32.9% 对 1.0%)相比,这些聚类解释了参与时间变化的更大比例,并且对参与时间的预测更准确(均方根误差:4.29 对 5.21,平均绝对误差:3.30 对 4.26)。
参与基于手机的数字活动的提供者对教学内容有内在的偏好。 与基于人口统计学变量的目标相比,基于个体内容偏好的目标可能会导致更高的提供者参与度。