Department of Otorhinolaryngology and Head and Neck Surgery, Erasmus Medical Center, Sophia Children's Hospital, Rotterdam, The Netherlands.
Department of Otorhinolaryngology, Erasmus Medical Center, Sophia Children's Hospital, Room SP-1421a, Rotterdam, The Netherlands.
Eur Arch Otorhinolaryngol. 2020 Jun;277(6):1725-1731. doi: 10.1007/s00405-020-05877-0. Epub 2020 Mar 4.
Prolonged endotracheal intubation may lead to laryngeal damage, with stridor being the most relevant clinical symptom. Our objective was to determine the incidence of post-extubation stridor and their clinical consequences in children within a tertiary referral center and to identify contributing factors.
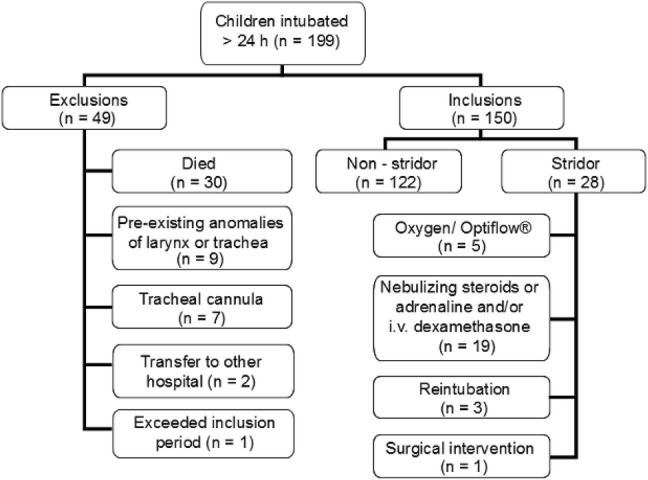
150 children, aged 0-16 years, intubated for more than 24 h were prospectively enrolled until discharge of the hospital. Potential relevant factors, thought to mediate the risk of laryngeal damage, were recorded and analyzed.
The median duration of intubation was 4 days, ranging from 1 to 31 days. Stridor following extubation occurred in 28 patients (18.7%); 3 of them required reintubation due to respiratory distress and in 1 child stridor persisted for which a surgical intervention was necessary. In multivariate analyses, we found the following independent predictors of stridor: intubation on the scene, the use of cuffed tubes and lower age.
Despite a high incidence for post-extubation stridor, only few children need reintubation or surgical intervention as a result of post-extubation lesions. Intubation on the scene, the use of cuffed tubes and young age are associated with a significant increased risk of post-extubation stridor. Awareness of these factors gives the possibility to anticipate on the situation and to minimize laryngeal injury and its possible future consequences.
长时间的气管插管可能导致喉部损伤,其中喘鸣是最相关的临床症状。我们的目的是确定在一家三级转诊中心中,拔管后喘鸣的发生率及其在儿童中的临床后果,并确定其相关因素。
150 名年龄在 0-16 岁之间、插管时间超过 24 小时的儿童前瞻性入组,直至出院。记录并分析了可能导致喉损伤的潜在相关因素。
插管时间中位数为 4 天,范围为 1 至 31 天。28 名患者(18.7%)在拔管后出现喘鸣;其中 3 名因呼吸困难需要再次插管,1 名儿童的喘鸣持续存在,需要手术干预。多变量分析发现,以下因素是喘鸣的独立预测因素:现场插管、使用带套囊的导管和年龄较小。
尽管拔管后喘鸣的发生率较高,但只有少数儿童因拔管后损伤而需要再次插管或手术干预。现场插管、使用带套囊的导管和年龄较小与拔管后喘鸣的风险显著增加相关。了解这些因素可以预测这种情况,并尽量减少喉部损伤及其可能的未来后果。