Kim Hongsun, Cho Yang Hyun
Department of Thoracic and Cardiovascular surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Acute Crit Care. 2020 Feb;35(1):1-9. doi: 10.4266/acc.2020.00080. Epub 2020 Feb 29.
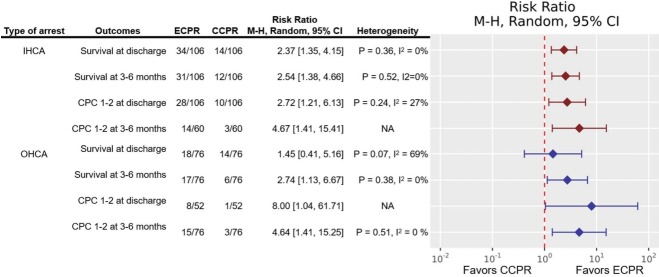
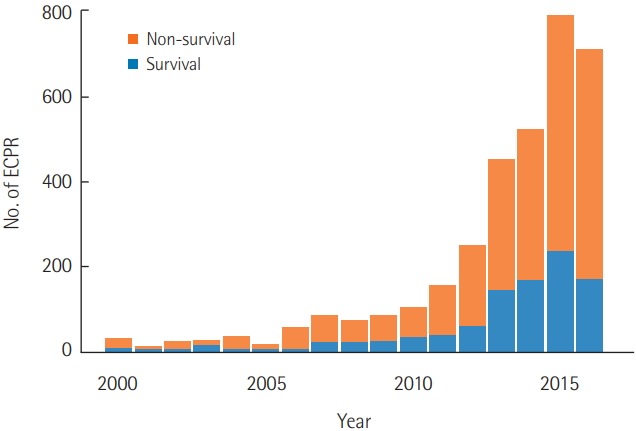
Extracorporeal cardiopulmonary resuscitation (ECPR) has been performed with increasing frequency worldwide to improve the low survival rate of conventional cardiopulmonary resuscitation (CCPR). Several studies have shown that among patients who experience in-hospital cardiac arrest, better survival outcomes and neurological outcomes can be expected after ECPR than after CCPR. However, studies have not clearly shown a short-term survival benefit of ECPR for patients who experience out-of-hospital cardiac arrest. Favorable outcomes are associated with a shorter low-flow time, an initial shockable rhythm, lower serum lactate levels, higher blood pH, and a lower Sequential Organ Failure Assessment score. Indications for ECPR include young age, witnessed arrest with bystander cardiopulmonary resuscitation, an initial shockable rhythm, correctable causes such as a cardiac etiology, and no return of spontaneous circulation within 10-20 minutes of CCPR. ECPR is a complex intervention that requires a highly trained team, specialized equipment, and multidisciplinary support within a healthcare system, and it has the risk of several life-threatening complications. Therefore, physicians should carefully select patients for ECPR who can gain the most benefit, instead of applying ECPR indiscriminately.
体外心肺复苏(ECPR)在全球范围内的实施频率不断增加,以改善传统心肺复苏(CCPR)较低的生存率。多项研究表明,在发生院内心脏骤停的患者中,与CCPR相比,ECPR后有望获得更好的生存结局和神经学结局。然而,研究尚未明确显示ECPR对院外心脏骤停患者有短期生存益处。良好的结局与较短的低血流时间、初始可电击心律、较低的血清乳酸水平、较高的血液pH值以及较低的序贯器官衰竭评估评分相关。ECPR的适应症包括年轻、有旁观者进行心肺复苏的目击骤停、初始可电击心律、可纠正的病因(如心脏病因)以及CCPR 10 - 20分钟内无自主循环恢复。ECPR是一种复杂的干预措施,需要训练有素的团队、专门的设备以及医疗系统内的多学科支持,并且存在多种危及生命并发症的风险。因此,医生应谨慎选择能从ECPR中获益最大的患者,而不是盲目应用ECPR。