Mokin Maxim, Primiani Christopher T, Castonguay Alicia C, Nogueira Raul G, Haussen Diogo C, English Joey D, Satti Sudhakar R, Chen Jennifer, Farid Hamed, Borders Candace, Veznedaroglu Erol, Binning Mandy J, Puri Ajit, Vora Nirav A, Budzik Ron F, Dabus Guilherme, Linfante Italo, Janardhan Vallabh, Alshekhlee Amer, Abraham Michael G, Edgell Randall, Taqi Muhammad Asif, Khoury Ramy El, Majjhoo Aniel Q, Kabbani Mouhammed R, Froehler Michael T, Finch Ira, Ansari Sameer A, Novakovic Roberta, Nguyen Thanh N, Zaidat Osama O
Department of Neurosurgery and Brain Repair, University of South Florida, Tampa, FL, United States.
Department of Neurology, University of Toledo, Toledo, OH, United States.
Front Neurol. 2020 Feb 18;11:83. doi: 10.3389/fneur.2020.00083. eCollection 2020.
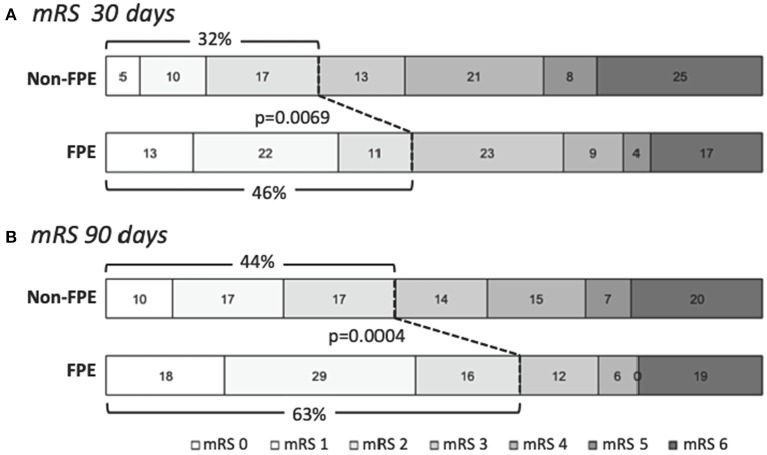
The first pass effect (FPE; achieving complete recanalization with a single thrombectomy device pass) has been shown to be associated with higher rates of good clinical outcomes in patients with acute ischemic stroke. Here, we investigate clinical and radiographic factors associated with FPE in a large U.S. post-marketing registry (TRACK, Trevo Stent-Retriever Acute Stroke). We analyzed the TRACK database (multicenter registry of 634 patients from 23 centers from March 2013 through August 2015), which 609 patients were included in the final analysis. FPE was defined as a single pass/use of device, TICI 2c/3 recanalization, and no use of rescue therapy. Analysis of individual patient data from TRACK were performed to analyze clinical and radiographic characteristics associated with FPE as well-compared clinical outcomes defined as modified Rankin Scale (mRS) score at 30 and 90 days from hospital discharge to the non-FPE group. The rate of FPE in TRACK was 23% (140/609). There was no association between patient demographics and FPE, including age ( = 0.36), sex ( = 0.50), race ( = 0.50), location of occlusion ( = 0.26), baseline NIHSS ( = 0.62), or past medical history. There was no difference in the use of a balloon-guide catheter or general anesthesia (49 and 57% with FPE vs. 47 and 64%, = 0.63 and = 0.14, respectively). Clinical outcomes were significantly associated with FPE; 63 vs. 44% in non-FPE patients achieved mRS 0-2 at 90 days ( = 0.0004). Our study showed that achieving complete recanalization with a single thrombectomy pass using the Trevo device was highly beneficial. The most common clinical factors that are used to determine eligibility for endovascular therapy, such as NIHSS severity, location of occlusion or patient age were not predictive of the ability to achieve FPE.
首次通过效应(FPE;使用单个血栓切除术装置一次通过实现完全再通)已被证明与急性缺血性中风患者更高的良好临床结局发生率相关。在此,我们在美国一个大型上市后注册研究(TRACK,Trevo支架取栓急性中风研究)中调查与FPE相关的临床和影像学因素。我们分析了TRACK数据库(2013年3月至2015年8月来自23个中心的634例患者的多中心注册研究),最终分析纳入了609例患者。FPE定义为装置单次通过/使用、TICI 2c/3级再通且未使用补救治疗。对TRACK中个体患者数据进行分析,以分析与FPE相关的临床和影像学特征,并比较出院后30天和90天改良Rankin量表(mRS)评分定义的临床结局与非FPE组。TRACK中的FPE发生率为23%(140/609)。患者人口统计学特征与FPE之间无关联,包括年龄(P = 0.36)、性别(P = 0.50)、种族(P = 0.50)、闭塞部位(P = 0.26)、基线美国国立卫生研究院卒中量表(NIHSS)评分(P = 0.62)或既往病史。使用球囊导引导管或全身麻醉方面无差异(FPE组分别为49%和57%,非FPE组分别为47%和64%,P分别为0.63和0.14)。临床结局与FPE显著相关;非FPE患者90天时mRS评分为0 - 2的比例为44%,而FPE患者为63%(P = 0.0004)。我们的研究表明,使用Trevo装置单次取栓实现完全再通非常有益。用于确定血管内治疗 eligibility 的最常见临床因素,如NIHSS严重程度、闭塞部位或患者年龄,并不能预测实现FPE的能力。 (注:原文中“eligibility”一词在句中语义似乎不完整,可能影响对整体内容的理解,但按照要求未添加额外解释。)