Scrutinio Domenico, Battista Petronilla, Guida Pietro, Lanzillo Bernardo, Tortelli Rosanna
Department of Neurorehabilitation, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy.
Department of Neurodegenerative Disease, University College London (UCL) Institute of Neurology, London, United Kingdom.
Front Neurol. 2020 Feb 18;11:84. doi: 10.3389/fneur.2020.00084. eCollection 2020.
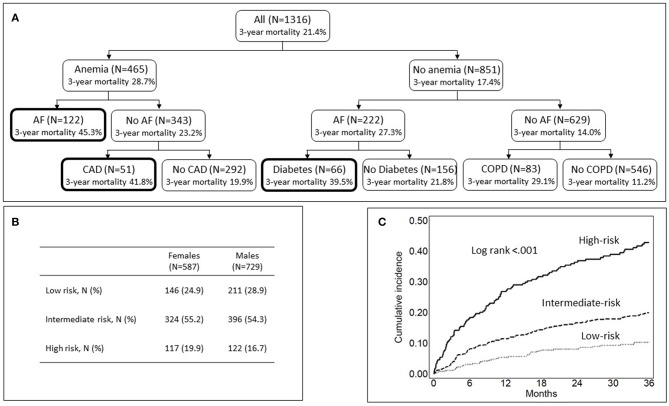
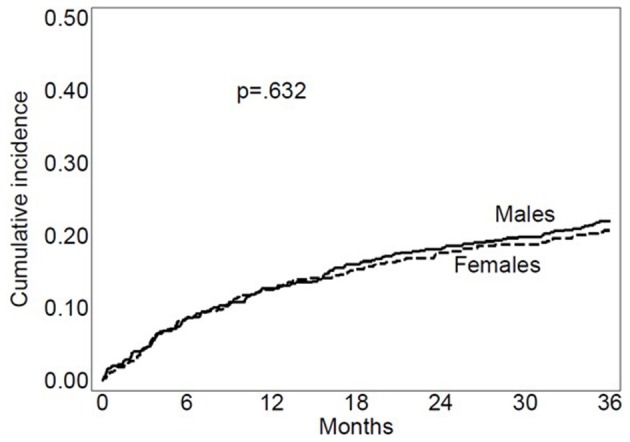
We sought to determine sex differences in outcomes in patients with severe stroke who had been admitted to inpatient rehabilitation. We studied 1,316 patients aged 18 to 99 (mean 72) classified as case-mix groups 0108, 0109, and 0110 of the Medicare case-mix classification system. These groups encompass the most severe strokes. Three outcomes were analyzed: (1) 3-year mortality from admission to rehabilitation; (2) combined outcome of transfer to acute care or death within 90 days from admission to rehabilitation; (3) functional outcome, including proportional recovery in motor functioning and good functional outcome as defined by achievement of a Functional Independence Measure (FIM)-motor score ≥65 points at discharge. Multivariable regression analyses were used to assess sex-difference in each outcome between women and men. The covariates examined included age, marital status, comorbidities, time from stroke onset to rehabilitation admission <30 days, ischemic stroke, dysphagia, neglect, motor FIM score at admission, and cognitive FIM score at admission. Kaplan-Meier estimated 3-year mortality rate was 20.7% in women and 22.0% in men. The crude hazard ratio (HR) of death for women compared with men was 0.94 (95% CI 0.74-1.20). After adjustment for significant covariates, the HR of 3-year mortality was 0.73 (95% CIs 0.56-0.96; = 0.025). Comorbidity, including diabetes, anemia, coronary artery disease, atrial fibrillation, and chronic obstructive pulmonary disease, significantly increased mortality risk by 49-88%. The incidence of the combined outcome was 8.3% in women and 8.4% in men. The crude HR of the combined end-point for women compared with men was 1.05 (95% CI 0.72-1.53). After adjustment for significant covariates, the HR was 0.95 (95% CIs 0.65-1.40; = 0.810). Likewise, no significant difference in proportional recovery or in the rate of achievement of a good functional outcome between women and men was observed. Among patients admitted to inpatient rehabilitation after severe stroke, women and men had comparable crude mortality rates at 3 years. After multivariable adjustment, however, women had lower mortality risk. No sex-differences in the risk of being transferred to acute care or dying within 90 days from admission to rehabilitation or in responsiveness to rehabilitation were observed.
我们试图确定入住住院康复机构的重症中风患者的预后性别差异。我们研究了1316名年龄在18至99岁(平均72岁)的患者,这些患者被归类为医疗保险病例组合分类系统的病例组合组0108、0109和0110。这些组包含最严重的中风病例。分析了三个预后指标:(1)从入院康复到3年的死亡率;(2)从入院康复到90天内转至急性护理或死亡的综合预后;(3)功能预后,包括运动功能的比例恢复以及出院时功能独立性测量(FIM)运动评分≥65分所定义的良好功能预后。采用多变量回归分析评估女性和男性在各预后指标上的性别差异。所检查的协变量包括年龄、婚姻状况、合并症、中风发作至康复入院时间<30天、缺血性中风、吞咽困难、偏侧忽视、入院时的运动FIM评分以及入院时的认知FIM评分。Kaplan-Meier估计女性3年死亡率为20.7%,男性为22.0%。女性与男性相比的粗死亡风险比(HR)为0.94(95%CI 0.74 - 1.20)。在对显著协变量进行调整后,3年死亡率的HR为0.73(95%CI 0.56 - 0.96;P = 0.025)。合并症,包括糖尿病、贫血、冠状动脉疾病、心房颤动和慢性阻塞性肺疾病,使死亡风险显著增加49% - 88%。综合预后的发生率女性为8.3%,男性为8.4%。女性与男性相比的综合终点粗HR为1.05(95%CI 0.72 - 1.53)。在对显著协变量进行调整后,HR为0.95(95%CI 0.65 - 1.40;P = 0.810)。同样,未观察到女性和男性在比例恢复或良好功能预后达成率方面的显著差异。在重症中风后入住住院康复机构的患者中,女性和男性3年的粗死亡率相当。然而,经过多变量调整后,女性的死亡风险较低。未观察到从入院康复到90天内转至急性护理或死亡风险或康复反应方面的性别差异。