Neurosurgery, University of Alabama at Birmingham, Birmingham, Alabama, USA.
Program for Global Surgery and Social Change, Harvard Medical School Department of Global Health and Social Medicine, Boston, Massachusetts, USA.
BMJ Glob Health. 2020 Feb 23;5(2):e002100. doi: 10.1136/bmjgh-2019-002100. eCollection 2020.
Managing paediatric hydrocephalus with shunt placement is especially risky in resource-limited settings due to risks of infection and delayed life-threatening shunt obstruction. This study evaluated a new evidence-based treatment algorithm to reduce shunt-dependence in this context.
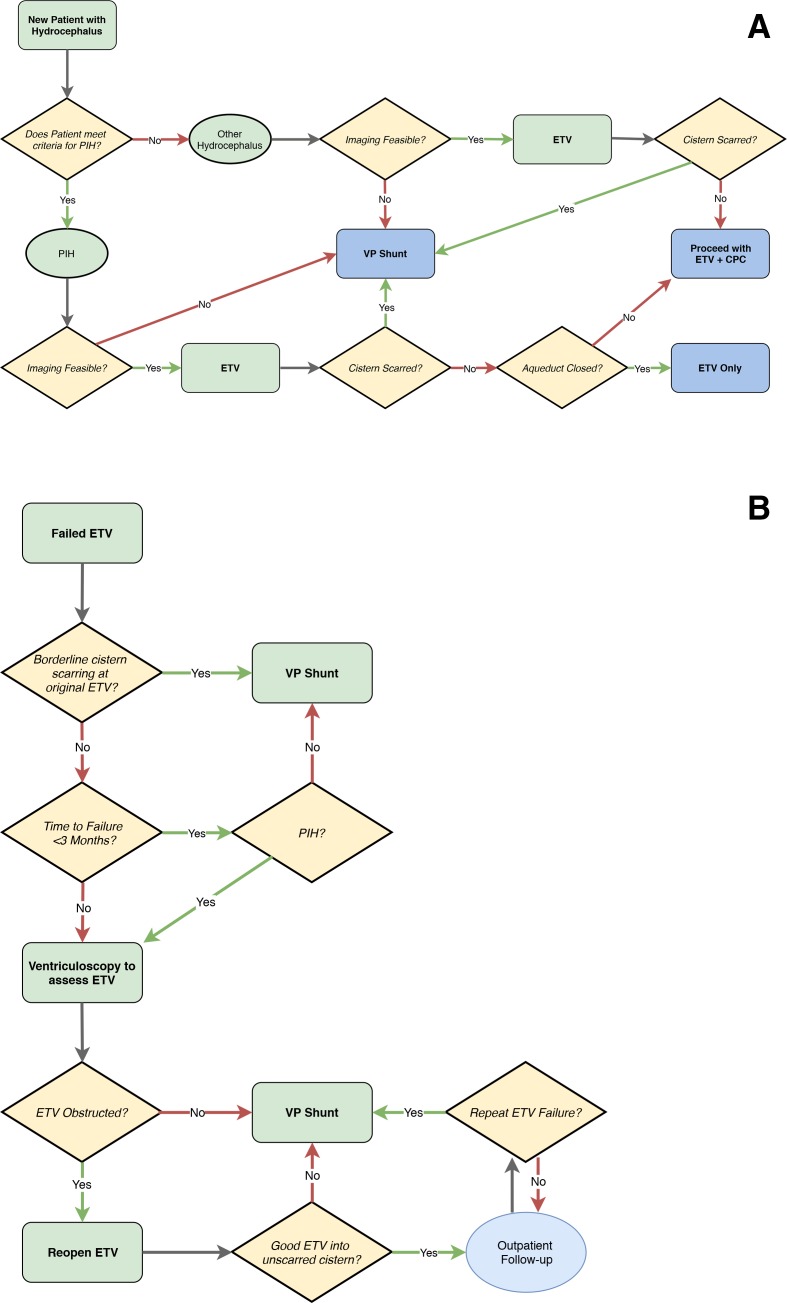
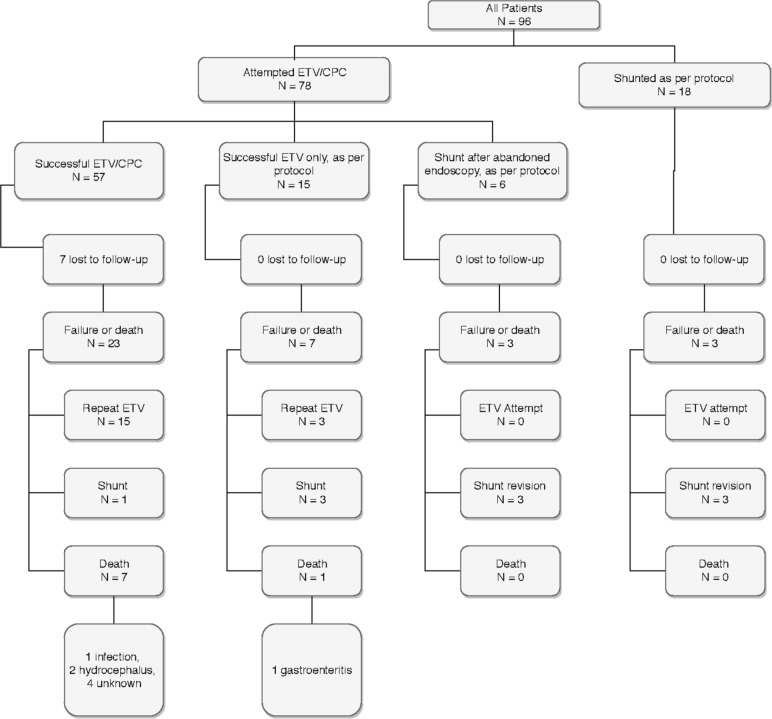
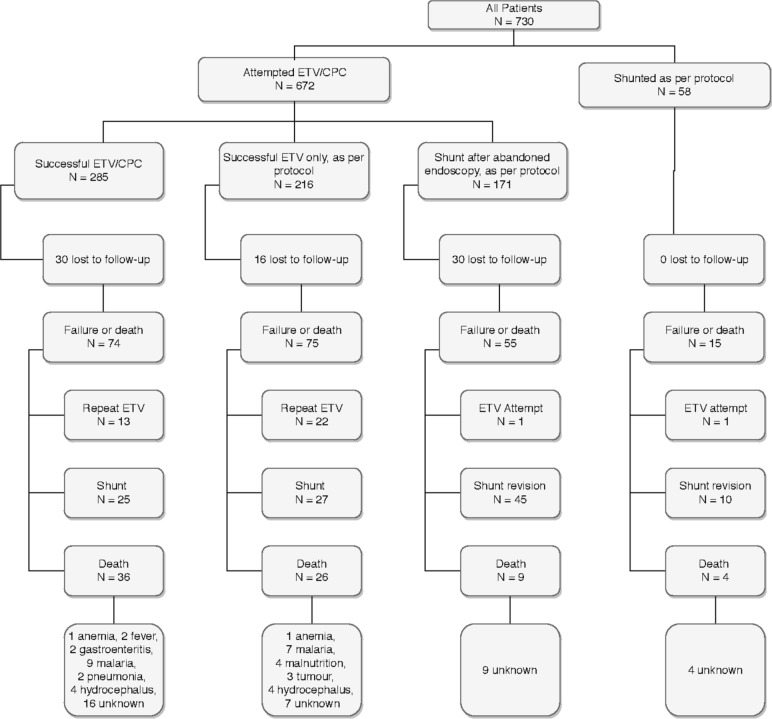
A prospective cohort design was used. The CURE Protocol employs preoperative and intraoperative data to choose between endoscopic treatment and shunt placement. Data were prospectively collected for 730 children in Uganda (managed by local neurosurgeons highly experienced in the protocol) and, for external validation, 96 children in Nigeria (managed by a local neurosurgeon trained in the protocol).
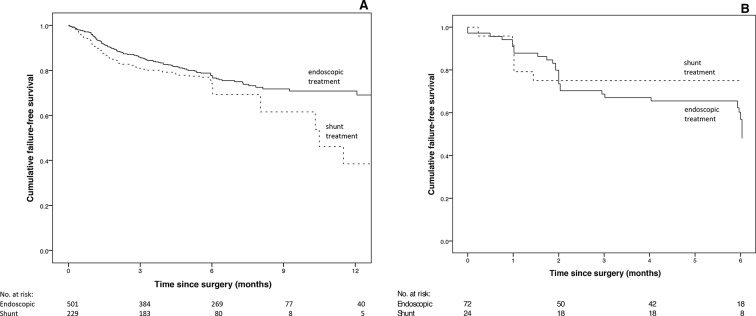
The age distribution was similar between Uganda and Nigeria, but there were more cases of postinfectious hydrocephalus in Uganda (64.2% vs 26.0%, p<0.001). Initial treatment of hydrocephalus was similar at both centres and included either a shunt at first operation or endoscopic management without a shunt. The Nigerian cohort had a higher failure rate for endoscopic cases (adjusted HR 2.5 (95% CI 1.6 to 4.0), p<0.001), but not for shunt cases (adjusted HR 1.3 (0.5 to 3.0), p=0.6). Despite the difference in endoscopic failure rates, a similar proportion of the entire cohort was successfully treated without need for shunt at 6 months (55.2% in Nigeria vs 53.4% in Uganda, p=0.74).
Use of the CURE Protocol in two centres with different populations and surgeon experience yielded similar 6-month results, with over half of all children remaining shunt-free. Where feasible, this could represent a better public health strategy in low-resource settings than primary shunt placement.
在资源有限的环境中,通过放置分流管来治疗小儿脑积水尤其具有风险,因为存在感染和延迟危及生命的分流管阻塞的风险。本研究评估了一种新的基于证据的治疗方案,以减少这种情况下对分流管的依赖。
采用前瞻性队列设计。CURE 方案利用术前和术中数据来选择内镜治疗或分流管放置。前瞻性收集了乌干达 730 名儿童(由对该方案具有丰富经验的当地神经外科医生管理)的数据,并对尼日利亚 96 名儿童(由接受过该方案培训的当地神经外科医生管理)进行了外部验证。
乌干达和尼日利亚的年龄分布相似,但乌干达的感染后脑积水病例更多(64.2%比 26.0%,p<0.001)。两个中心的初始脑积水治疗方法相似,包括首次手术时放置分流管或不放置分流管的内镜治疗。尼日利亚队列中内镜治疗失败率更高(调整后的 HR 2.5(95%CI 1.6 至 4.0),p<0.001),但分流治疗失败率无差异(调整后的 HR 1.3(0.5 至 3.0),p=0.6)。尽管内镜治疗失败率存在差异,但在 6 个月时,整个队列中无需分流管成功治疗的比例相似(尼日利亚为 55.2%,乌干达为 53.4%,p=0.74)。
在具有不同人群和外科医生经验的两个中心使用 CURE 方案,得出了相似的 6 个月结果,超过一半的儿童无需分流管。在可行的情况下,与初次放置分流管相比,这在资源有限的环境中可能是一种更好的公共卫生策略。