Kulkarni Abhaya V, Schiff Steven J, Mbabazi-Kabachelor Edith, Mugamba John, Ssenyonga Peter, Donnelly Ruth, Levenbach Jody, Monga Vishal, Peterson Mallory, MacDonald Michael, Cherukuri Venkateswararao, Warf Benjamin C
From the University of Toronto (A.V.K.) and the Hospital for Sick Children (A.V.K., R.D., J.L.), Toronto; Pennsylvania State University, University Park (S.J.S., V.M., M.P., M.M., V.C.); CURE Children's Hospital of Uganda, Mbale (E.M.-K., J.M., P.S., B.C.W.); and Harvard Medical School and Boston Children's Hospital, Boston (B.C.W.).
N Engl J Med. 2017 Dec 21;377(25):2456-2464. doi: 10.1056/NEJMoa1707568.
Postinfectious hydrocephalus in infants is a major health problem in sub-Saharan Africa. The conventional treatment is ventriculoperitoneal shunting, but surgeons are usually not immediately available to revise shunts when they fail. Endoscopic third ventriculostomy with choroid plexus cauterization (ETV-CPC) is an alternative treatment that is less subject to late failure but is also less likely than shunting to result in a reduction in ventricular size that might facilitate better brain growth and cognitive outcomes.
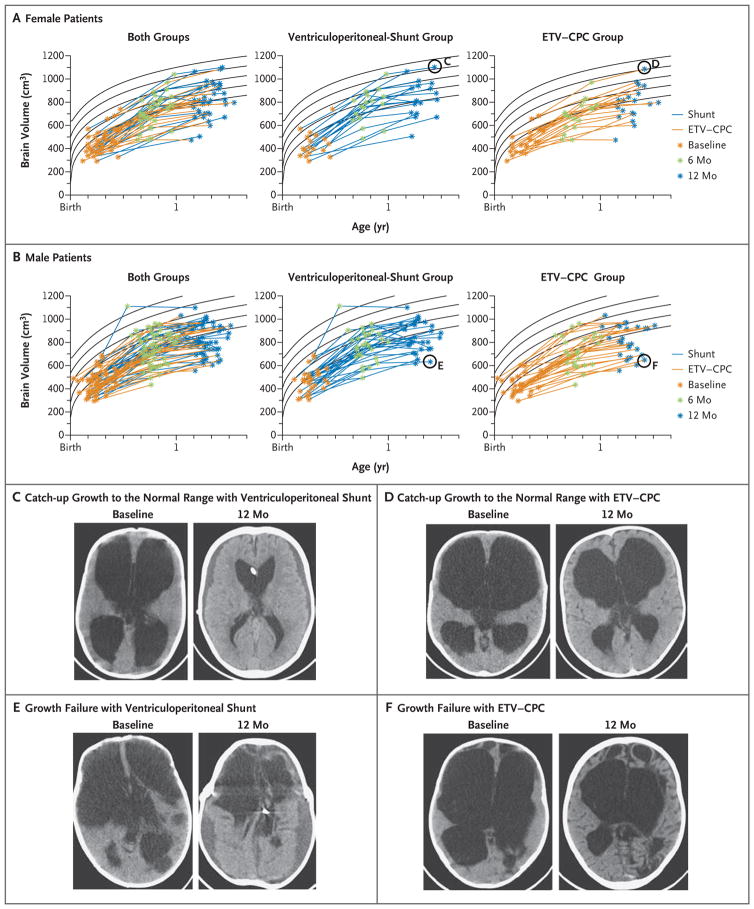
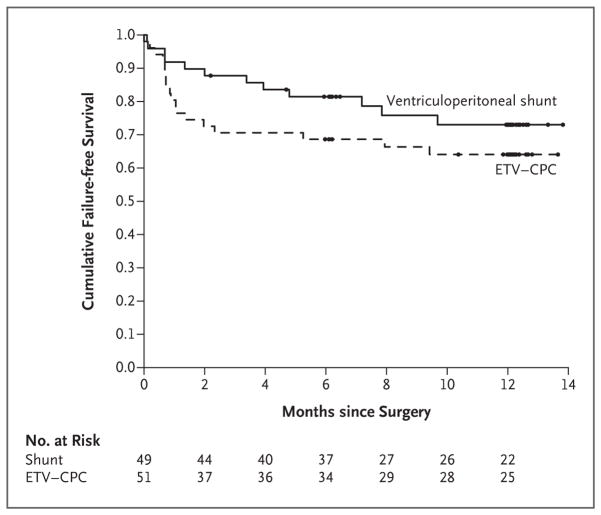
We conducted a randomized trial to evaluate cognitive outcomes after ETV-CPC versus ventriculoperitoneal shunting in Ugandan infants with postinfectious hydrocephalus. The primary outcome was the Bayley Scales of Infant Development, Third Edition (BSID-3), cognitive scaled score 12 months after surgery (scores range from 1 to 19, with higher scores indicating better performance). The secondary outcomes were BSID-3 motor and language scores, treatment failure (defined as treatment-related death or the need for repeat surgery), and brain volume measured on computed tomography.
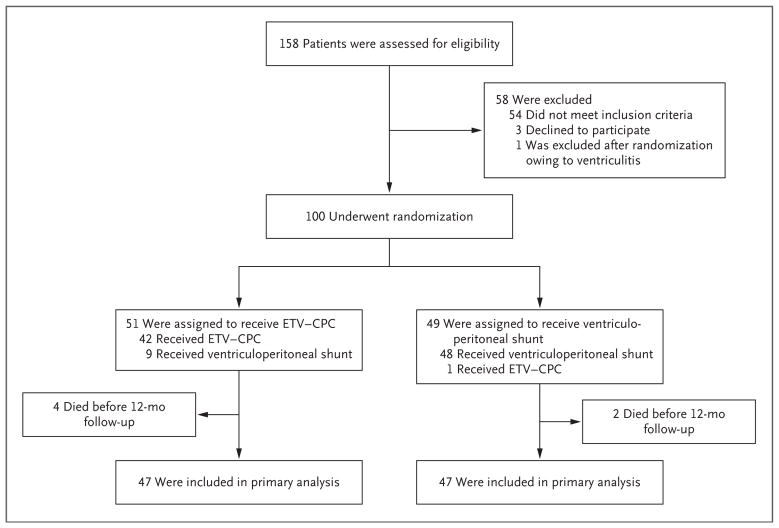
A total of 100 infants were enrolled; 51 were randomly assigned to undergo ETV-CPC, and 49 were assigned to undergo ventriculoperitoneal shunting. The median BSID-3 cognitive scores at 12 months did not differ significantly between the treatment groups (a score of 4 for ETV-CPC and 2 for ventriculoperitoneal shunting; Hodges-Lehmann estimated difference, 0; 95% confidence interval [CI], -2 to 0; P=0.35). There was no significant difference between the ETV-CPC group and the ventriculoperitoneal-shunt group in BSID-3 motor or language scores, rates of treatment failure (35% and 24%, respectively; hazard ratio, 0.7; 95% CI, 0.3 to 1.5; P=0.24), or brain volume (z score, -2.4 and -2.1, respectively; estimated difference, 0.3; 95% CI, -0.3 to 1.0; P=0.12).
This single-center study involving Ugandan infants with postinfectious hydrocephalus showed no significant difference between endoscopic ETV-CPC and ventriculoperitoneal shunting with regard to cognitive outcomes at 12 months. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT01936272 .).
婴儿感染后脑积水是撒哈拉以南非洲地区的一个主要健康问题。传统治疗方法是脑室腹腔分流术,但当分流失败时,外科医生通常无法立即进行修复手术。内镜下第三脑室造瘘术联合脉络丛烧灼术(ETV-CPC)是一种替代治疗方法,其后期失败的可能性较小,但与分流术相比,导致脑室缩小从而促进更好的脑发育和认知结果的可能性也较小。
我们进行了一项随机试验,以评估乌干达感染后脑积水婴儿接受ETV-CPC与脑室腹腔分流术后的认知结果。主要结局是贝利婴幼儿发展量表第三版(BSID-3)术后12个月的认知量表评分(评分范围为1至19分,分数越高表明表现越好)。次要结局包括BSID-3运动和语言评分、治疗失败(定义为与治疗相关的死亡或需要再次手术)以及计算机断层扫描测量的脑容量。
共纳入100名婴儿;51名被随机分配接受ETV-CPC,49名被分配接受脑室腹腔分流术。治疗组之间术后12个月的BSID-3认知评分中位数无显著差异(ETV-CPC组评分为4分,脑室腹腔分流术组评分为2分;霍奇斯-莱曼估计差异为0;95%置信区间[CI],-2至0;P=0.35)。ETV-CPC组与脑室腹腔分流术组在BSID-3运动或语言评分、治疗失败率(分别为35%和24%;风险比,0.7;95%CI,0.3至1.5;P=0.24)或脑容量(z评分分别为-2.4和-2.1;估计差异为0.3;95%CI,-0.3至1.0;P=0.12)方面均无显著差异。
这项涉及乌干达感染后脑积水婴儿的单中心研究表明,内镜下ETV-CPC与脑室腹腔分流术在术后12个月的认知结果方面无显著差异。(由美国国立卫生研究院资助;ClinicalTrials.gov编号,NCT01936272。)