Department of Radiation Biology, Centre for Cancer and Organ Diseases, Rigshospitalet, Copenhagen, Denmark.
Department of Oncology, Centre for Cancer and Organ Diseases, Rigshospitalet, Copenhagen, Denmark.
Mol Oncol. 2020 May;14(5):964-973. doi: 10.1002/1878-0261.12660. Epub 2020 Mar 18.
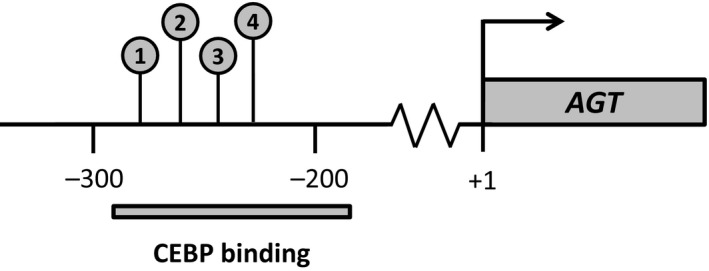
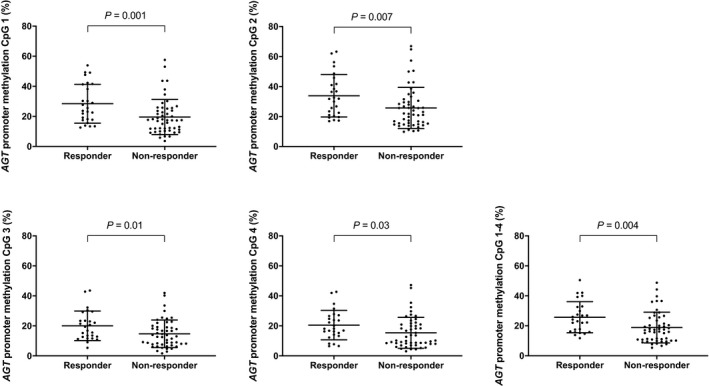
Patients with recurrent glioblastoma achieving response to bevacizumab combined with chemotherapy have clinical improvement and prolonged survival. High gene expression of angiotensinogen (AGT) is associated with a poor bevacizumab response. Because AGT expression is epigenetically regulated, we aimed to investigate whether AGT promoter methylation in tumor tissue predicts response to bevacizumab combination therapy in patients with recurrent glioblastoma. The study included 159 patients with recurrent glioblastoma, treated with bevacizumab combination treatment (training cohort, n = 77; validation cohort, n = 82). All patients could be evaluated for treatment response and biomarkers. DNA methylation of 4 CpG sites in the AGT promoter was measured using pyrosequencing. A model for nonresponse was established using logistic regression analysis. In the training cohort, lower methylation of each of the four CpG sites in the AGT promoter was significantly associated with nonresponse (all P < 0.05). Moreover, the mean methylation level of all four CpG sites was associated with an increased likelihood of not achieving response to bevacizumab combination therapy (twofold decrease: odds ratio = 3.01; 95% confidence interval: 1.41-6.44; P = 0.004). We developed a model for nonresponse in the training cohort, where a threshold of mean AGT promoter methylation levels was set to below 12%. The model could predict bevacizumab nonresponse with 96% specificity. Importantly, this predictor was also significantly associated with nonresponse in the validation cohort (P = 0.037). Taken together, our findings suggest that low AGT promoter methylation in tumor tissue predicts nonresponse to bevacizumab combination treatment in patients with recurrent glioblastoma. We have, thus, established and successfully validated a predictor for nonresponse that can be used to identify patients who will not benefit from bevacizumab combination therapy.
接受贝伐珠单抗联合化疗治疗后出现缓解的复发性胶质母细胞瘤患者具有临床改善和延长的生存时间。血管紧张素原(AGT)的高基因表达与贝伐珠单抗反应不良相关。由于 AGT 表达受表观遗传调控,我们旨在研究肿瘤组织中 AGT 启动子甲基化是否可预测复发性胶质母细胞瘤患者对贝伐珠单抗联合治疗的反应。该研究纳入了 159 例接受贝伐珠单抗联合治疗的复发性胶质母细胞瘤患者(训练队列,n=77;验证队列,n=82)。所有患者均可评估治疗反应和生物标志物。采用焦磷酸测序法测量 AGT 启动子中 4 个 CpG 位点的 DNA 甲基化。使用逻辑回归分析建立无应答模型。在训练队列中,AGT 启动子中每个 CpG 位点的低甲基化与无应答显著相关(均 P<0.05)。此外,所有 4 个 CpG 位点的平均甲基化水平与无法实现贝伐珠单抗联合治疗应答的可能性增加相关(降低 2 倍:比值比=3.01;95%置信区间:1.41-6.44;P=0.004)。我们在训练队列中建立了无应答模型,将 AGT 启动子甲基化水平的阈值设定在 12%以下。该模型可预测贝伐珠单抗无应答,特异性为 96%。重要的是,该预测指标在验证队列中也与无应答显著相关(P=0.037)。综上所述,我们的研究结果表明,肿瘤组织中 AGT 启动子的低甲基化可预测复发性胶质母细胞瘤患者对贝伐珠单抗联合治疗的无应答。我们已建立并成功验证了一种无应答预测指标,可用于识别不能从贝伐珠单抗联合治疗中获益的患者。