Urology Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Health Economics and Outcomes Research, Pharmerit International, Bethesda, MD, USA.
J Sex Med. 2020 May;17(5):941-948. doi: 10.1016/j.jsxm.2020.01.027. Epub 2020 Mar 3.
While phosphodiesterase type-5 inhibitors (PDE5Is) are highly effective for the treatment of erectile dysfunction (ED) and well tolerated, updated data on prescription patterns have been limited in real-world settings.
To describe men in the United States who are prescribed PDE5Is for ED treatment and to evaluate patterns of initiation, switching, and treatment overlap.
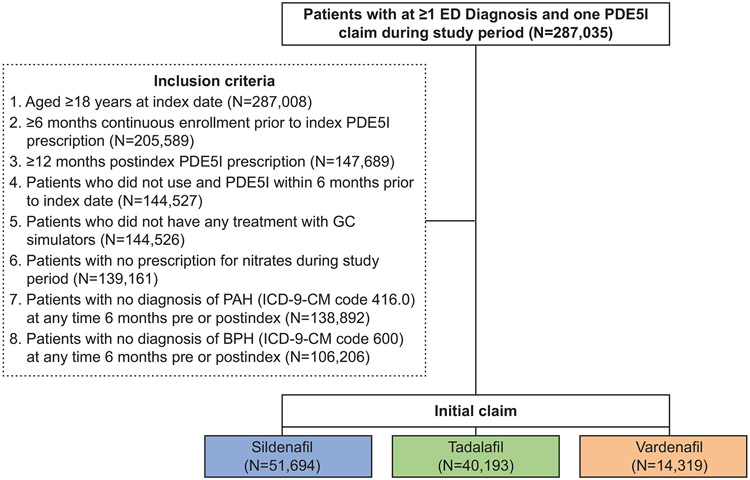
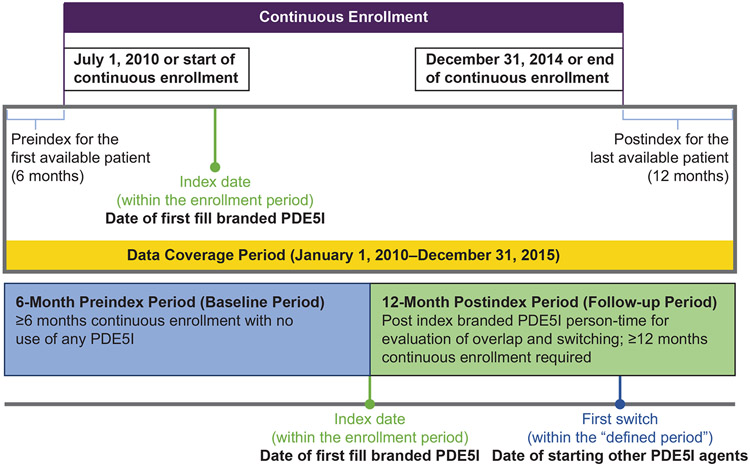
This retrospective claims study used MarketScan Commercial and Medicare Supplement Databases from January 1, 2010, to December 31, 2015, to identify initial PDE5I claims (index date) for sildenafil, tadalafil, and/or vardenafil. Adults aged ≥18 years with ED were identified between July 1, 2010, and December 31, 2014, allowing for a 6-month preindex and 12-month follow-up period from the index date.
Outcomes included patient demographics and treatment-related patterns after treatment initiation.
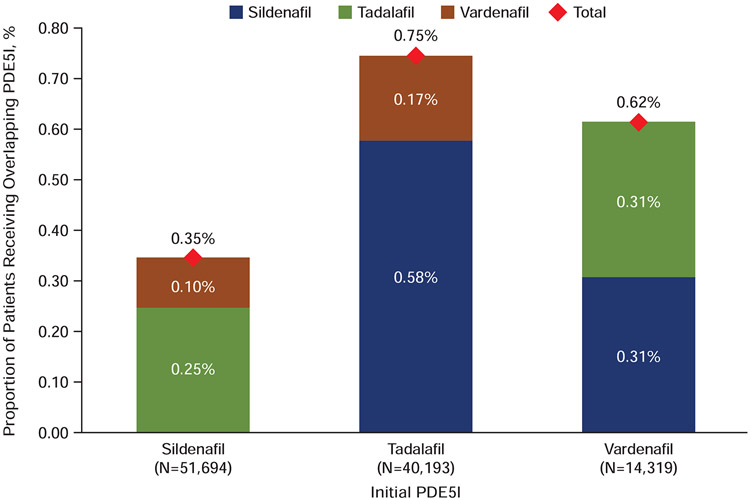
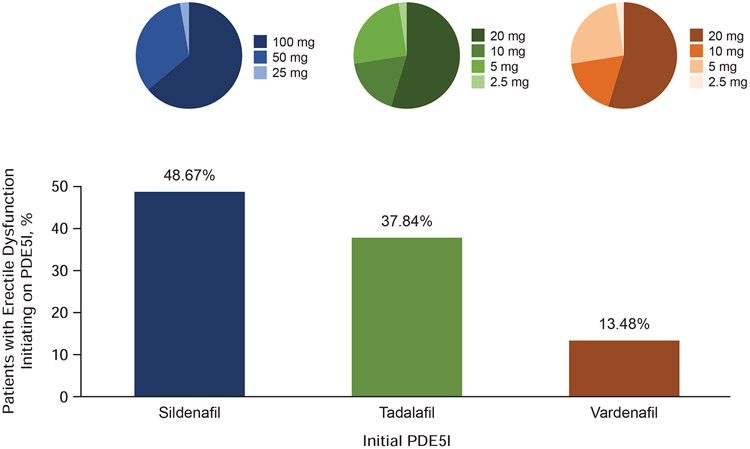
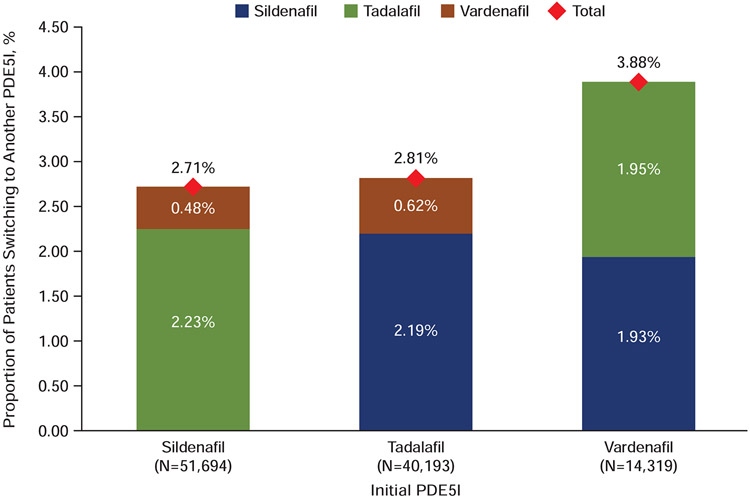
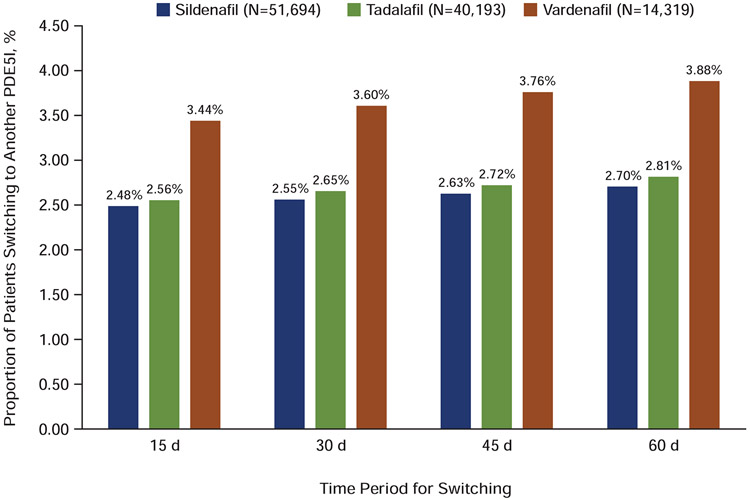
A total of 106,206 identified patients met all inclusion criteria. Of these, 51,694, 40,193, and 14,319 had initial claims for sildenafil, tadalafil, and vardenafil, respectively. Mean age was 50.35 years, and comorbidities included dyslipidemia (44.17%), hypertension (43.09%), diabetes (15.32%), and depression (10.61%). More patients (48.67%) initiated on sildenafil than tadalafil (37.85%) or vardenafil (13.48%). Rate of switching was lower in the 60 days after the end of day supply of the initial prescription in the sildenafil cohort (2.71%) compared with the tadalafil (2.81%) and vardenafil (3.88%) cohorts (P < .001 for sildenafil vs tadalafil or vardenafil). Treatment overlap was lower in the sildenafil cohort (0.35%) than in the tadalafil (0.75%) and vardenafil (0.62%) groups (P < .001 for sildenafil vs tadalafil or vardenafil).
These findings provide insight into updated patterns of PDE5I prescriptions in the United States and may aid in clinical decision-making.
STRENGTHS & LIMITATIONS: Strengths include the large sample size, long data coverage period, and the real-world nature of the study. Limitations include the retrospective study design, use of data collected with a primary focus of claims, and lack of further details regarding reasons that drive switching. Actual rates of ED and impact on prescription patterns may be underestimated because the claims database only captured patients electing to visit a health-care provider.
Among men with ED in the United States, rates of switching and treatment overlap were low for all PDE5Is but were found to be the lowest for sildenafil compared with tadalafil and vardenafil. Mulhall JP, Chopra I, Patel D, et al. Phosphodiesterase Type-5 Inhibitor Prescription Patterns in the United States Among Men With Erectile Dysfunction: An Update. J Sex Med 2020;17:941-948.
磷酸二酯酶 5 型抑制剂(PDE5Is)在治疗勃起功能障碍(ED)方面非常有效,且耐受性良好,但在真实世界环境中,关于处方模式的最新数据有限。
描述美国开具 PDE5Is 治疗 ED 的男性患者,并评估起始、转换和治疗重叠模式。
这项回顾性索赔研究使用 MarketScan 商业和医疗保险补充数据库,时间范围为 2010 年 1 月 1 日至 2015 年 12 月 31 日,以确定西地那非、他达拉非和/或伐地那非的初始 PDE5I 索赔(索引日期)。2010 年 7 月 1 日至 2014 年 12 月 31 日期间确定患有 ED 的年龄≥18 岁的成年人,允许从索引日期前 6 个月和 12 个月的随访期。
共确定了 106206 名符合所有纳入标准的患者。其中,51694 名、40193 名和 14319 名患者分别首次使用西地那非、他达拉非和伐地那非。平均年龄为 50.35 岁,合并症包括血脂异常(44.17%)、高血压(43.09%)、糖尿病(15.32%)和抑郁症(10.61%)。与他达拉非(37.85%)或伐地那非(13.48%)相比,更多的患者(48.67%)起始使用西地那非。在西地那非组中,初始处方结束后的 60 天内,换药率(2.71%)低于他达拉非组(2.81%)和伐地那非组(3.88%)(西地那非与他达拉非或伐地那非比较,P<.001)。与他达拉非(0.75%)和伐地那非(0.62%)组相比,西地那非组的治疗重叠率(0.35%)较低(西地那非与他达拉非或伐地那非比较,P<.001)。
这些发现提供了关于美国 PDE5I 处方最新模式的见解,可能有助于临床决策。
优势包括样本量大、数据覆盖时间长、研究的真实世界性质。局限性包括回顾性研究设计、主要关注索赔收集的数据使用,以及缺乏进一步的详细信息,无法了解驱动换药的原因。由于索赔数据库仅捕获了选择就诊的患者,ED 的实际发病率和对处方模式的影响可能被低估。
在美国患有 ED 的男性中,所有 PDE5Is 的换药率和治疗重叠率均较低,但与他达拉非和伐地那非相比,西地那非的比例最低。