Melbourne School of Population and Global Health, The University of Melbourne, Carlton, Victoria, Australia.
The George Institute for Global Health, UNSW Sydney, Newtown, New South Wales, 2042, Australia.
BMC Med. 2020 Mar 9;18(1):60. doi: 10.1186/s12916-020-01520-1.
The majority of low- and middle-income countries (LMICs) do not have adequate civil registration and vital statistics (CRVS) systems to properly support health policy formulation. Verbal autopsy (VA), long used in research, can provide useful information on the cause of death (COD) in populations where physicians are not available to complete medical certificates of COD. Here, we report on the application of the SmartVA tool for the collection and analysis of data in several countries as part of routine CRVS activities.
Data from VA interviews conducted in 4 of 12 countries supported by the Bloomberg Philanthropies Data for Health (D4H) Initiative, and at different stages of health statistical development, were analysed and assessed for plausibility: Myanmar, Papua New Guinea (PNG), Bangladesh and the Philippines. Analyses by age- and cause-specific mortality fractions were compared to the Global Burden of Disease (GBD) study data by country. VA interviews were analysed using SmartVA-Analyze-automated software that was designed for use in CRVS systems. The method in the Philippines differed from the other sites in that the VA output was used as a decision support tool for health officers.
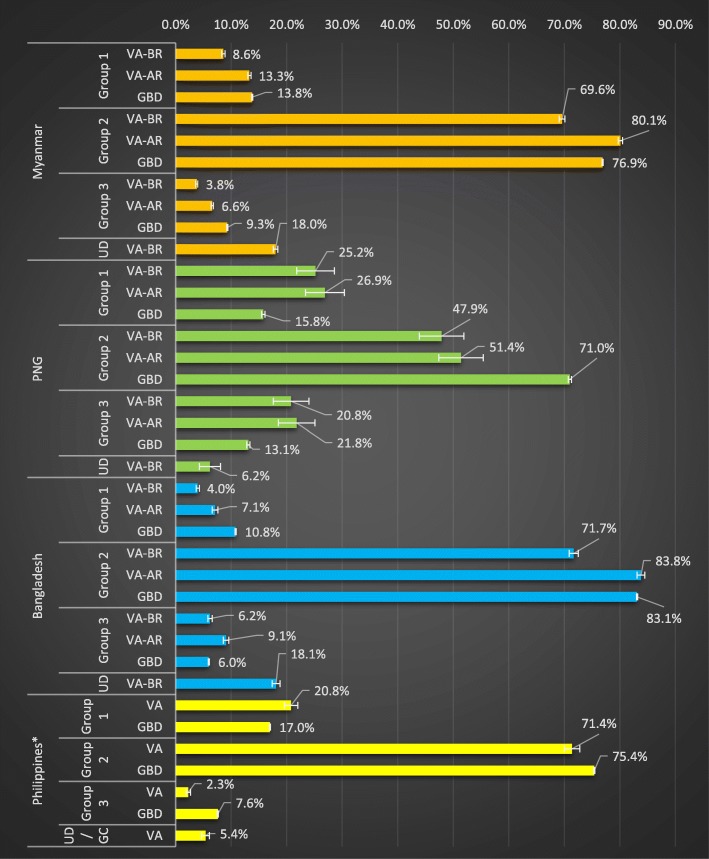
Country strategies for VA implementation are described in detail. Comparisons between VA data and country GBD estimates by age and cause revealed generally similar patterns and distributions. The main discrepancy was higher infectious disease mortality and lower non-communicable disease mortality at the PNG VA sites, compared to the GBD country models, which critical appraisal suggests may highlight real differences rather than implausible VA results.
Automated VA is the only feasible method for generating COD data for many populations. The results of implementation in four countries, reported here under the D4H Initiative, confirm that these methods are acceptable for wide-scale implementation and can produce reliable COD information on community deaths for which little was previously known.
大多数中低收入国家(LMICs)没有足够的民事登记和生命统计(CRVS)系统来正确支持卫生政策的制定。尸检(VA)长期以来一直用于研究,可以为无法完成医生死亡原因医学证明的人群提供有关死亡原因(COD)的有用信息。在这里,我们报告了 SmartVA 工具在几个国家/地区的应用,该工具用于收集和分析数据,作为常规 CRVS 活动的一部分。
对彭博慈善基金会健康数据(D4H)倡议支持的 12 个国家中的 4 个国家(缅甸、巴布亚新几内亚(PNG)、孟加拉国和菲律宾)进行的 VA 访谈数据进行了分析和评估,这些国家处于不同的健康统计发展阶段:分析了年龄和病因特异性死亡率分数,并与按国家划分的全球疾病负担(GBD)研究数据进行了比较。VA 访谈使用专为 CRVS 系统设计的 SmartVA-Analyze-automated 软件进行分析。菲律宾的方法与其他地点不同,VA 输出被用作卫生官员的决策支持工具。
详细描述了 VA 实施的国家战略。VA 数据与国家 GBD 估计数按年龄和病因的比较显示出相似的模式和分布。主要差异是 PNG VA 站点的传染病死亡率较高,而非传染性疾病死亡率较低,与 GBD 国家模型相比,这表明批判性评估可能突出了真实的差异,而不是不合理的 VA 结果。
自动 VA 是为许多人群生成 COD 数据的唯一可行方法。这里在 D4H 倡议下报告的四个国家的实施结果证实,这些方法可以广泛实施,并可以为先前知之甚少的社区死亡提供可靠的 COD 信息。