Tian Ya-Li, Ji Jing-Jing, Chen Lu-Ning, Cui Xin-Long, Liu Shi-Teng, Mao Liang, Qiu Yu-Dong, Li Bing-Bing
Department of Anesthesiology, Drum Tower Hospital Affiliated with the Nanjing University Medical School, Nanjing 210008, Jiangsu Province, China.
Department of Surgery, Division of Hepatobiliary and Pancreatic Surgery, Drum Tower Hospital Affiliated with the Nanjing University Medical School, Nanjing 210008, Jiangsu Province, China.
World J Clin Cases. 2020 Feb 26;8(4):713-722. doi: 10.12998/wjcc.v8.i4.713.
The risk factors for patients with major postoperative complications immediately after liver resection have been identified; however, the intermediate and long-term prognoses for these patients have yet to be determined.
To evaluate the factors responsible for the long-term recurrence-free survival rate in patients with hepatocellular carcinoma (HCC) following anatomic hepatectomy.
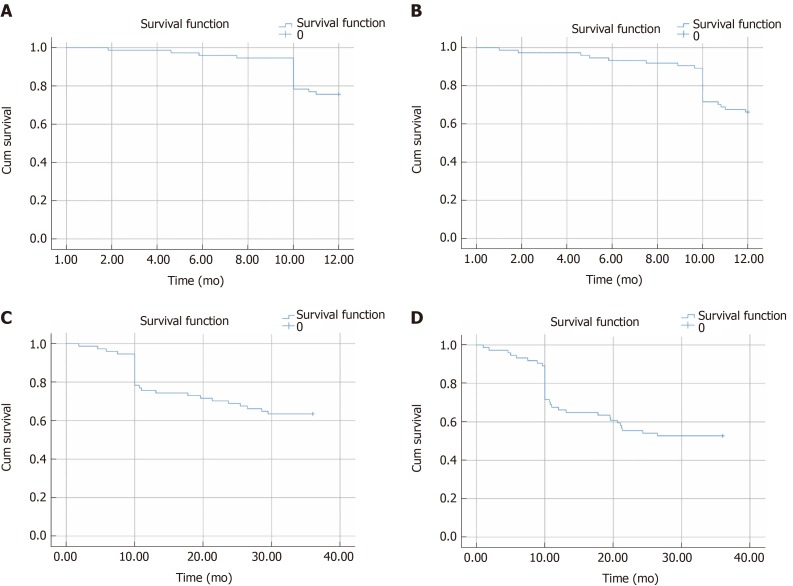
We performed a retrospective analysis of 74 patients with HCC who underwent precise anatomic hepatectomy at our institution from January 2013 to December 2015. The observational endpoints for this study were the tumor recurrence or death of the HCC patients. The overall follow-up duration was three years. The recurrence-free survival curves were plotted by the Kaplan-Meier method and were analyzed by the log-rank test. The value of each variable for predicting prognosis was assessed multivariate Cox proportional hazards regression analysis.
The 1-year and 3-year recurrence-free survival rates of HCC patients were 68.92% and 55.41%, respectively, following anatomic liver resection. The results showed that the 3-year recurrence-free survival rate in HCC patients was closely related to preoperative cirrhosis, jaundice level, tumor stage, maximal tumor diameter, complications of diabetes mellitus, frequency of intraoperative hypotensive episodes, estimated blood loss (EBL), blood transfusion, fluid infusion, and postoperative infection ( < 0.1). Based on multivariate analysis, preoperative cirrhosis, tumor stage, intraoperative hypotension, and EBL were identified to be predictors of 3-year recurrence-free survival in HCC patients undergoing anatomic hepatectomy ( < 0.05).
Tumor stage and preoperative cirrhosis adversely affect the recurrence-free survival rate in HCC patients following anatomic hepatectomy. The long-term recurrence-free survival rate of patients with HCC is closely related to intraoperative hypotension and EBL.
肝切除术后即刻发生严重术后并发症患者的危险因素已得到确认;然而,这些患者的中长期预后仍有待确定。
评估肝细胞癌(HCC)患者解剖性肝切除术后长期无复发生存率的相关因素。
我们对2013年1月至2015年12月在我院接受精确解剖性肝切除的74例HCC患者进行了回顾性分析。本研究的观察终点为HCC患者的肿瘤复发或死亡。总随访时间为3年。采用Kaplan-Meier法绘制无复发生存曲线,并通过对数秩检验进行分析。通过多因素Cox比例风险回归分析评估每个变量对预后的预测价值。
解剖性肝切除术后,HCC患者的1年和3年无复发生存率分别为68.92%和55.41%。结果显示,HCC患者的3年无复发生存率与术前肝硬化、黄疸水平、肿瘤分期、最大肿瘤直径、糖尿病并发症、术中低血压发作频率、估计失血量(EBL)、输血、液体输注及术后感染密切相关(P<0.1)。基于多因素分析,术前肝硬化、肿瘤分期、术中低血压及EBL被确定为接受解剖性肝切除的HCC患者3年无复发生存率的预测因素(P<0.05)。
肿瘤分期和术前肝硬化对解剖性肝切除术后HCC患者的无复发生存率有不利影响。HCC患者的长期无复发生存率与术中低血压及EBL密切相关。