Srinivas Nithya, Barbour April M, Epstein Noam, Zhou Gongfu, Petusky Susan, Xun Zhinyin, Yuska Brad, Marbury Thomas, Chen Xuejun, Yeleswaram Swamy, Punwani Naresh
Incyte Corporation, Wilmington, Delaware, USA.
Orlando Clinical Research Center, Orlando, Florida, USA.
J Clin Pharmacol. 2020 Aug;60(8):1022-1029. doi: 10.1002/jcph.1601. Epub 2020 Mar 9.
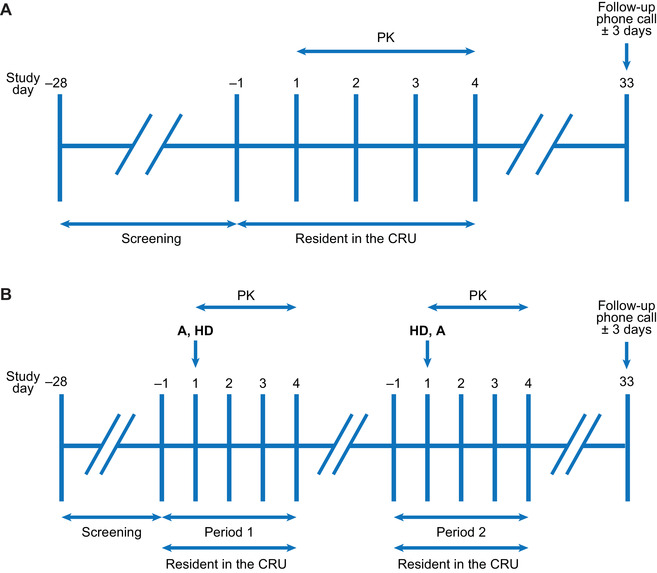
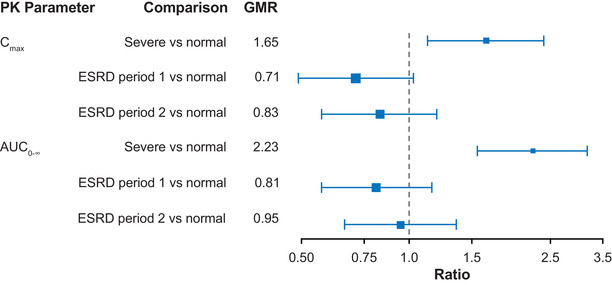
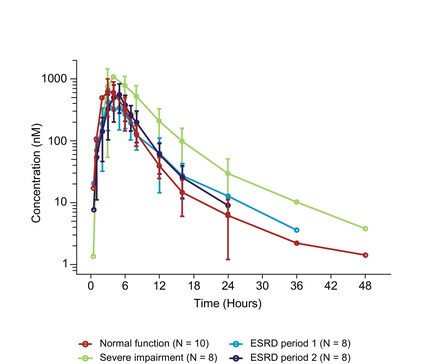
Itacitinib is a novel, selective, Janus kinase 1 inhibitor in development for treatment of graft-versus-host disease. The objective of this study was to assess pharmacokinetics and safety of 300-mg itacitinib dosed in participants with normal renal function (n = 10), severe renal impairment (n = 8), and end-stage renal disease (ESRD) on hemodialysis (n = 8). Serial plasma and urine samples (urine from normal and severe groups only) were collected before dosing until 72 hours after dosing. In the ESRD group, itacitinib was evaluated in 2 periods, when dosed before (period 1) and after (period 2) a hemodialysis session. Geometric mean ratios (90% confidence interval) in participants with severe renal impairment, ESRD period 1 and ESRD period 2 relative to participants with normal renal function were 1.65 (1.13-2.39), 0.71 (0.49-1.03), and 0.83 (0.57-1.20) for maximum plasma drug concentration and 2.23 (1.56-3.18), 0.81 (0.57-1.16), and 0.95 (0.66-1.35) for area under the plasma concentration-time curve from time zero to infinity. Itacitinib was well tolerated, and 3 grade 1 treatment-emergent adverse events were reported over the course of the study. Given the magnitude of exposure changes in participants with severe renal impairment or ESRD and the historic risk-benefit profile, no dose adjustment is recommended for itacitinib in patients with impaired renal function, although the final dosage recommendation will be based on cumulative pharmacokinetics and safety from this study and from the pivotal graft-versus-host disease trial. Additionally, itacitinib may be administered to patients undergoing dialysis regardless of the time of dialysis.
伊他西替尼是一种新型、选择性的 Janus 激酶 1 抑制剂,正处于治疗移植物抗宿主病的研发阶段。本研究的目的是评估 300mg 伊他西替尼在肾功能正常的参与者(n = 10)、严重肾功能损害者(n = 8)和接受血液透析的终末期肾病(ESRD)患者(n = 8)中的药代动力学和安全性。在给药前直至给药后 72 小时收集系列血浆和尿液样本(仅正常组和严重组的尿液)。在 ESRD 组中,伊他西替尼在血液透析前(第 1 期)和血液透析后(第 2 期)两个时期进行评估。与肾功能正常的参与者相比,严重肾功能损害者、ESRD 第 1 期和 ESRD 第 2 期参与者的最大血浆药物浓度的几何平均比值(90%置信区间)分别为 1.65(1.13 - 2.39)、0.71(0.49 - 1.03)和 0.83(0.57 - 1.20),从零时间到无穷大的血浆浓度 - 时间曲线下面积的几何平均比值分别为 2.23(1.56 - 3.18)、0.81(0.57 - 1.16)和 0.9(0.66 - 1.35)。伊他西替尼耐受性良好,在研究过程中报告了 3 例 1 级治疗中出现的不良事件。鉴于严重肾功能损害或 ESRD 参与者的暴露变化程度以及既往的风险 - 获益情况,尽管最终剂量建议将基于本研究和关键的移植物抗宿主病试验的累积药代动力学和安全性,但不建议对肾功能受损患者调整伊他西替尼剂量。此外,无论透析时间如何,伊他西替尼均可用于接受透析的患者。