Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, New York.
now with College of Population Health, Thomas Jefferson University, Philadelphia, Pennsylvania.
JAMA Netw Open. 2020 Mar 2;3(3):e1919963. doi: 10.1001/jamanetworkopen.2019.19963.
Colorectal cancer (CRC) is the second leading cause of cancer-related mortality in the United States. The prognosis for patients with CRC varies widely, but new prognostic biomarkers provide the opportunity to implement a more individualized approach to treatment selection.
To assess the cost-effectiveness of 3 therapeutic strategies, namely, endoscopic therapy (ET), laparoscopic colectomy (LC), and open colectomy (OC), for patients with T1 CRC with biomarker profiles that prognosticate varying levels of tumor progression in the US payer perspective.
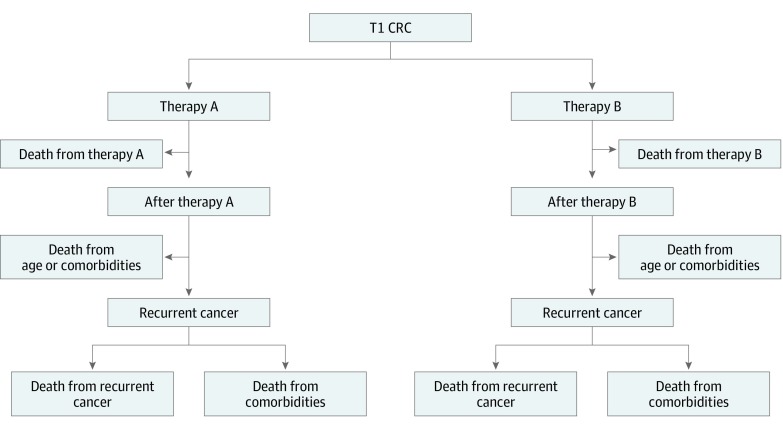
DESIGN, SETTING, AND PARTICIPANTS: In this economic evaluation study, a Markov model was developed for the cost-effectiveness analysis. Risks of all-cause mortality and recurrent cancer after ET, LC, or OC were estimated with a 35-year time horizon. Quality of life was based on EuroQoL 5 Dimensions scores reported in the published literature. Hospital and treatment costs reflected Medicare reimbursement rates. Deterministic and probabilistic sensitivity analyses were performed. Data from patients with T1 CRC and 6 biomarker profiles that included adenomatous polyposis coli (APC), TP53 and/or KRAS, or BRAFV600E were used as inputs for the model. Data analyses were conducted from February 27, 2019, to May 13, 2019.
Endoscopic therapy, LC, and OC.
The primary outcomes were unadjusted life-years, quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER) between competing treatment strategies.
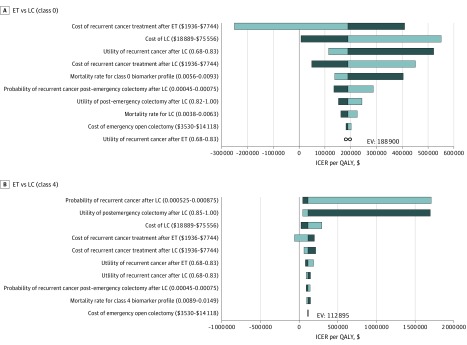
Endoscopic therapy had the highest QALYs and the lowest cost and was the dominant treatment strategy for T1 CRC with the following biomarker profiles: BRAFV600E, APC(1)/KRAS/TP53, APC(2) or APC(2)/KRAS or APC(2)/TP53, or APC(1) or APC(1)/KRAS or APC(1)/TP53. The QALYs gained ranged from 16.97 to 17.22, with costs between $68 902.75 and $77 784.53 in these subgroups. For the 2 more aggressive biomarker profiles with worse prognoses (APC(2)/KRAS/TP53 and APCwt [wild type]), LC was the most effective strategy (with 16.45 and 16.61 QALYs gained, respectively) but was not cost-effective. Laparoscopic colectomy cost $65 234.87 for APC(2)/KRAS/TP53 and $71 250.56 for APCwt, resulting in ICERs of $113 290 per QALY and $178 765 per QALY, respectively.
This modeling analysis found that ET was the most effective strategy for patients with T1 CRC with less aggressive biomarker profiles. For patients with more aggressive profiles, LC was more effective but was costly, rendering ET the cost-effective option. This study highlights the potential utility of prognostic biomarkers in T1 CRC treatment selection.
结直肠癌(CRC)是美国癌症相关死亡的第二大主要原因。CRC 患者的预后差异很大,但新的预后生物标志物为治疗选择实施更个体化的方法提供了机会。
从美国支付者的角度评估 3 种治疗策略(内镜治疗[ET]、腹腔镜结肠切除术[LC]和开腹结肠切除术[OC])在具有预测肿瘤进展程度不同水平的生物标志物特征的 T1 CRC 患者中的成本效益。
设计、地点和参与者:在这项经济评估研究中,开发了一个马尔可夫模型进行成本效益分析。使用 35 年的时间范围估计 ET、LC 或 OC 后所有原因死亡率和癌症复发的风险。基于文献中报告的 EuroQoL 5 维度评分来评估生活质量。医院和治疗费用反映了医疗保险报销率。进行了确定性和概率敏感性分析。使用 T1 CRC 患者的数据和 6 种生物标志物特征,包括腺瘤性息肉病 coli(APC)、TP53 和/或 KRAS 或 BRAFV600E,作为模型的输入。数据分析于 2019 年 2 月 27 日至 2019 年 5 月 13 日进行。
内镜治疗、LC 和 OC。
主要结局是未经调整的寿命年、质量调整寿命年(QALYs)和竞争治疗策略之间的增量成本效益比(ICER)。
内镜治疗具有最高的 QALYs 和最低的成本,并且是具有以下生物标志物特征的 T1 CRC 的主导治疗策略:BRAFV600E、APC(1)/KRAS/TP53、APC(2)或 APC(2)/KRAS 或 APC(2)/TP53,或 APC(1)或 APC(1)/KRAS 或 APC(1)/TP53。在这些亚组中,获得的 QALYs 范围为 16.97 至 17.22,成本为 68902.75 美元至 77784.53 美元。对于预后较差的 2 种更具侵袭性的生物标志物特征(APC(2)/KRAS/TP53 和 APCwt[野生型]),LC 是最有效的策略(分别获得 16.45 和 16.61 QALYs),但不具有成本效益。腹腔镜结肠切除术治疗 APC(2)/KRAS/TP53 的成本为 65234.87 美元,APCwt 的成本为 71250.56 美元,导致每 QALY 的 ICER 分别为 113290 美元和 178765 美元。
这项建模分析发现,对于具有侵袭性较小的生物标志物特征的 T1 CRC 患者,ET 是最有效的治疗策略。对于具有更具侵袭性特征的患者,LC 更有效但成本较高,使 ET 成为具有成本效益的选择。本研究强调了预后生物标志物在 T1 CRC 治疗选择中的潜在效用。