Advanced Emergency and Critical Care Center, Niigata University Medical & Dental Hospital, Niigata City, Niigata, Japan.
Department of Emergency & Critical Care Medicine, Niigata University Faculty of Medicine, Niigata City, Niigata, Japan.
PLoS One. 2020 Mar 9;15(3):e0229135. doi: 10.1371/journal.pone.0229135. eCollection 2020.
We performed an exclusive study to investigate the associations between a total of 23 lactate-related indices during the first 24h in an intensive care unit (ICU) and in-hospital mortality.
Nine static and 14 dynamic lactate indices, including changes in lactate concentrations (Δ Lac) and slope (linear regression coefficient), were calculated from individual critically ill patient data extracted from the Multiparameter Intelligent Monitoring for Intensive Care (MIMIC) III database.
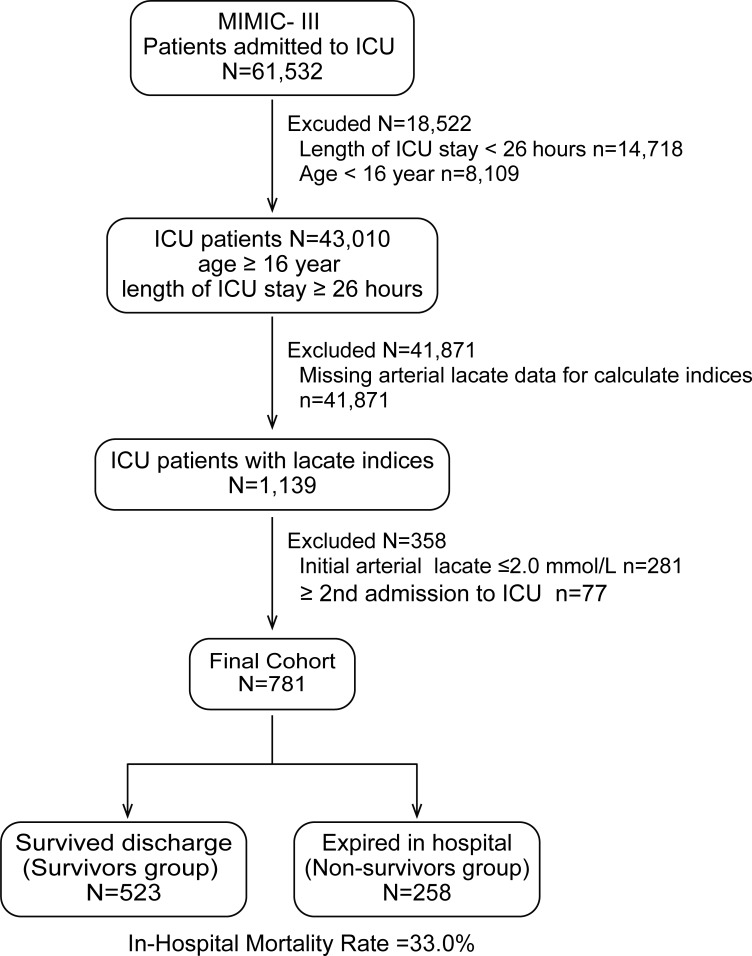
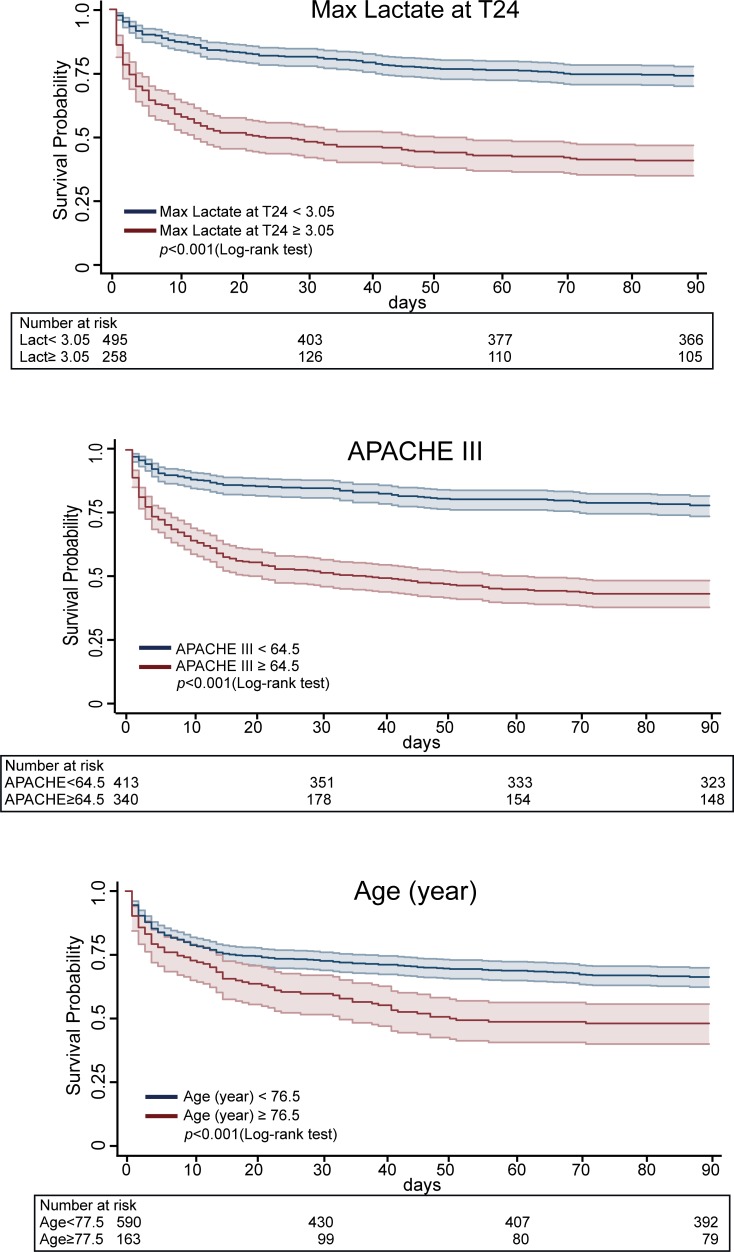
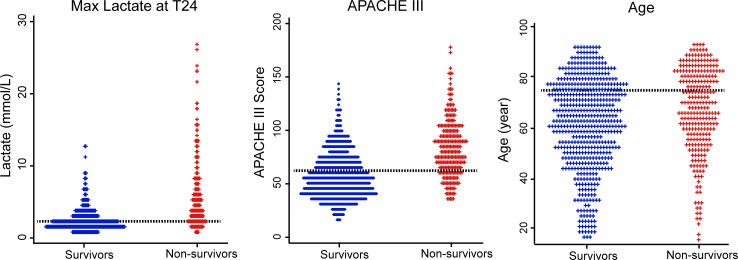
Data from a total of 781 ICU patients were extracted, consisted of 523 survivors and 258 non-survivors. The in-hospital mortality rate for this cohort was 33.0%. A multivariate logistic regression model identified maximal lactate concentration at 24h after ICU admission (max lactate at T24) as a significant predictor of in-hospital mortality (odds ratio = 1.431, 95% confidence interval [CI] = 1.278-1.604, p<0.001) after adjusting for predefined confounders (age, gender, sepsis, Elixhauser comorbidity score, mechanical ventilation, renal replacement therapy, vasopressors, ICU severity scores). Area under curve (AUC) for max lactate at T24 was larger (AUC = 0.776, 95% CI = 0.740-0.812) than other indices (p<0.001), comparable to an APACHE III score of 0.771. When combining max lactate at T24 with APACHE III, the AUC was increased to 0.815 (95% CI:0.783-0.847). The sensitivity, specificity, and positive and negative predictive values for the cut-off value of 3.05 mmol/L were 64.3%, 77.4%, 58.5%, and 81.5%, respectively. Kaplan-Myer survival curves of the max lactate at T24 for 90-day survival after admission to ICU demonstrated a significant difference according to the cut-off value (p<0.001).
These data indicate that the maximal arterial lactate concentration at T24 is a robust predictor of in-hospital mortality as well as 90-day survival in unselected ICU patients with predictive ability as comparable with APACHE III score.
我们进行了一项专门的研究,调查了重症监护病房(ICU)前 24 小时内总共 23 个乳酸相关指标与住院死亡率之间的关联。
从 Multiparameter Intelligent Monitoring for Intensive Care (MIMIC) III 数据库中提取个体危重症患者的数据,计算了 9 个静态乳酸指标和 14 个动态乳酸指标,包括乳酸浓度变化(Δ Lac)和斜率(线性回归系数)。
从总共 781 名 ICU 患者中提取数据,包括 523 名幸存者和 258 名非幸存者。该队列的住院死亡率为 33.0%。多变量逻辑回归模型确定 ICU 入院后 24 小时的最大乳酸浓度(max lactate at T24)是调整了年龄、性别、脓毒症、Elixhauser 合并症评分、机械通气、肾脏替代治疗、血管加压素、重症监护严重程度评分等预设混杂因素后住院死亡率的显著预测因子(比值比=1.431,95%置信区间[CI]:1.278-1.604,p<0.001)。max lactate at T24 的曲线下面积(AUC)较大(AUC=0.776,95%CI:0.740-0.812),优于其他指数(p<0.001),与 APACHE III 评分的 0.771 相当。当将 max lactate at T24 与 APACHE III 结合时,AUC 增加至 0.815(95%CI:0.783-0.847)。3.05mmol/L 截断值的灵敏度、特异性、阳性预测值和阴性预测值分别为 64.3%、77.4%、58.5%和 81.5%。根据截断值,max lactate at T24 的 ICU 入院后 90 天生存率 Kaplan-Meier 生存曲线显示出显著差异(p<0.001)。
这些数据表明,T24 时的最大动脉乳酸浓度是未选择的 ICU 患者住院死亡率和 90 天生存率的有力预测指标,预测能力与 APACHE III 评分相当。