Leidman Eva, Couture Alexia, Hulland Erin, Bilukha Oleg
Emergency Response and Recovery Branch, Division of Global Health Protection, Center for Global Health, Centers for Disease Control, 1600 Clifton Road, Atlanta, GA 30329 USA.
BMC Nutr. 2019 Aug 19;5:39. doi: 10.1186/s40795-019-0301-z. eCollection 2019.
Mid-upper arm circumference (MUAC) and weight-for-height (WHZ) are commonly used indicators to identify acute malnutrition. However, MUAC and WHZ diagnose different children, and produce prevalence estimates that are meaningfully different. Previous research in Somalia has suggested improved concordance using MUAC-for-age (MUACZ) rather than MUAC. We further evaluate the relationship between MUACZ, MUAC, and WHZ using surveys conducted globally.
We analyzed 882 population representative surveys from 41 countries. Children ages 6-59 months were classified as acutely malnourished using three independent criteria: WHZ < - 2 (WHZ2), MUAC< 125 mm (MUAC125), MUACZ < - 2 (MUACZ2). Population prevalence using each of the three criteria are presented by country and region. Correlations of survey prevalence for each indicator pair were assessed. Multivariable regression models of MUACZ and MUAC125 adjusted for WHZ2, stunting prevalence, age, and sex. To evaluate individual level diagnostic concordance, we compared the proportion of children identified by each of the three criteria.
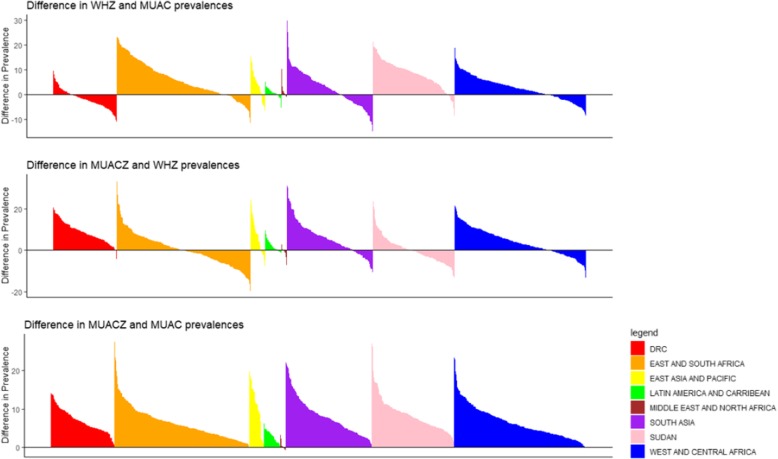
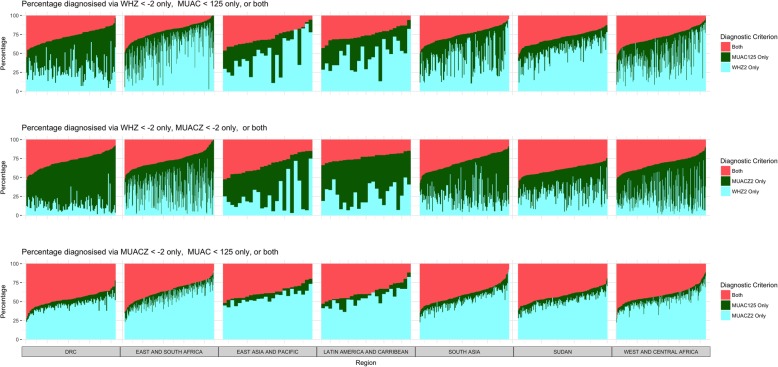
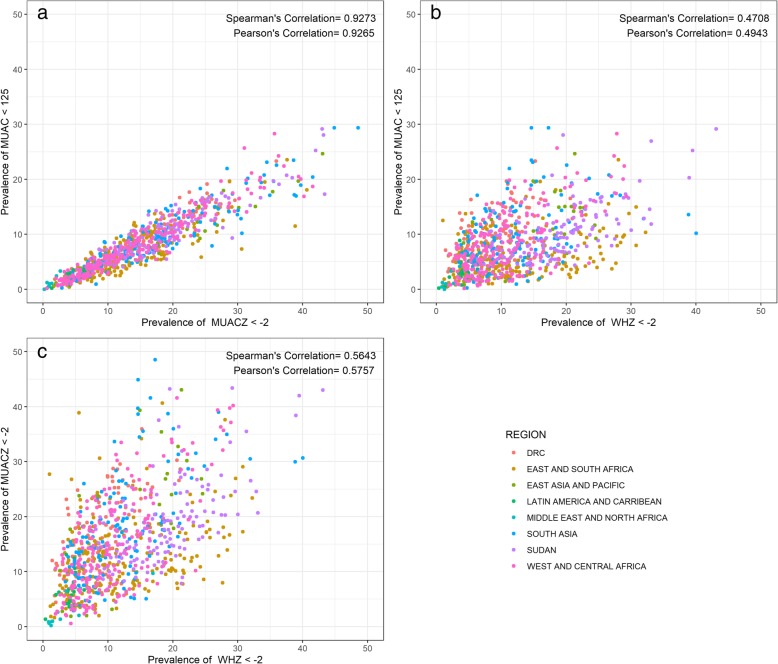
Median prevalence of acute malnutrition overall was highest for MUACZ2 (14.0%) followed by WHZ2 (10.6%), and lowest for MUAC125 (7.3%). The absolute difference in prevalence between MUACZ2 and WHZ2 was smaller than the difference between MUAC125 and WHZ2 for 51.3% of surveys. The correlations of WHZ2 with both MUACZ2 as well as with MUAC125 were weak, positive associations (Pearson's r = 0.5757 and 0.4943, respectively), but MUAC125 and MUACZ2 had a strong, linear relationship (Pearson's r = 0.9265). The adjusted regression model for MUACZ2 had greater fit (R = 0.50) relative to the adjusted model for MUAC125 (R = 0.43). The proportion of children identified by both MUAC125 and WHZ2 was 25.5%, smaller than the proportion identified by both MUACZ2 and WHZ2 (30.6%).
MUACZ identified more children as malnourished than MUAC, resulting in a higher prevalence of acute malnutrition in nearly all settings. Prevalence by MUACZ was not consistently more similar to WHZ than that estimated by MUAC, and correlations with WHZ were only slightly improved relative to MUAC. Consequently, programmatic use of MUACZ cannot be justified based on improved concordance with WHZ. Further research on morbidity and mortality of children with low MUACZ only are needed before recommending MUACZ for wider use.
上臂中部周长(MUAC)和身高别体重(WHZ)是用于识别急性营养不良的常用指标。然而,MUAC和WHZ诊断出的儿童不同,得出的患病率估计值也存在显著差异。此前在索马里的研究表明,使用年龄别上臂中部周长(MUACZ)而非MUAC可提高一致性。我们利用全球范围内开展的调查进一步评估MUACZ、MUAC和WHZ之间的关系。
我们分析了来自41个国家的882项具有人群代表性的调查。采用三个独立标准将6至59个月大的儿童分类为急性营养不良:WHZ<-2(WHZ2)、MUAC<125毫米(MUAC125)、MUACZ<-2(MUACZ2)。按国家和地区列出使用这三个标准各自得出的人群患病率。评估各指标对调查患病率的相关性。对MUACZ和MUAC125的多变量回归模型针对WHZ2、发育迟缓患病率、年龄和性别进行了调整。为评估个体水平的诊断一致性,我们比较了由这三个标准各自识别出的儿童比例。
总体而言,急性营养不良的患病率中位数以MUACZ2最高(14.0%),其次是WHZ2(10.6%),最低的是MUAC125(7.3%)。在51.3%的调查中,MUACZ2和WHZ2之间患病率的绝对差异小于MUAC125和WHZ2之间的差异。WHZ2与MUACZ2以及与MUAC125的相关性均较弱,呈正相关(皮尔逊r分别为0.5757和0.4943),但MUAC125和MUACZ2具有强线性关系(皮尔逊r = 0.9265)。相对于MUAC125的调整模型(R = 0.43),MUACZ2的调整回归模型拟合度更高(R = 0.50)。由MUAC125和WHZ2两者识别出的儿童比例为25.5%,小于由MUACZ2和WHZ2两者识别出的比例(30.6%)。
与MUAC相比,MUACZ识别出更多营养不良儿童,导致几乎在所有情况下急性营养不良的患病率更高。MUACZ得出的患病率与WHZ的一致性并不始终比MUAC估计的更相似,且与WHZ的相关性相对于MUAC仅略有改善。因此,基于与WHZ更好的一致性,无法证明在项目中使用MUACZ是合理的。在推荐更广泛使用MUACZ之前,仅需对MUACZ低的儿童的发病率和死亡率进行进一步研究。