Li Jieli, Chang Hui-Ming, Banchs Jose, Araujo Dejka M, Hassan Saamir A, Wagar Elizabeth A, Yeh Edward T H, Meng Qing H
1Department of Laboratory Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX USA.
2Center for Precision Medicine, Department of Medicine, University of Missouri School of Medicine, Columbia, MO USA.
Cardiooncology. 2020 Jan 2;6:1. doi: 10.1186/s40959-019-0056-3. eCollection 2020.
Continuous infusion of doxorubicin or dexrazoxane pre-treatment prior to bolus doxorubicin are proven strategies to protect against doxorubicin-induced cardiotoxicity. Recently, global longitudinal peak systolic strain (GLS) measured with speckle tracking echocardiography (STE) and high-sensitivity troponin T (hs-TnT) have been validated as sensitive indicators of doxorubicin-induced cardiotoxicity. Here, we asked whether changes in hs-TnT and/or GLS can be detected in patients who were treated with continuous infusion of doxorubicin or pre-treated with dexrazoxane followed by bolus doxorubicin.
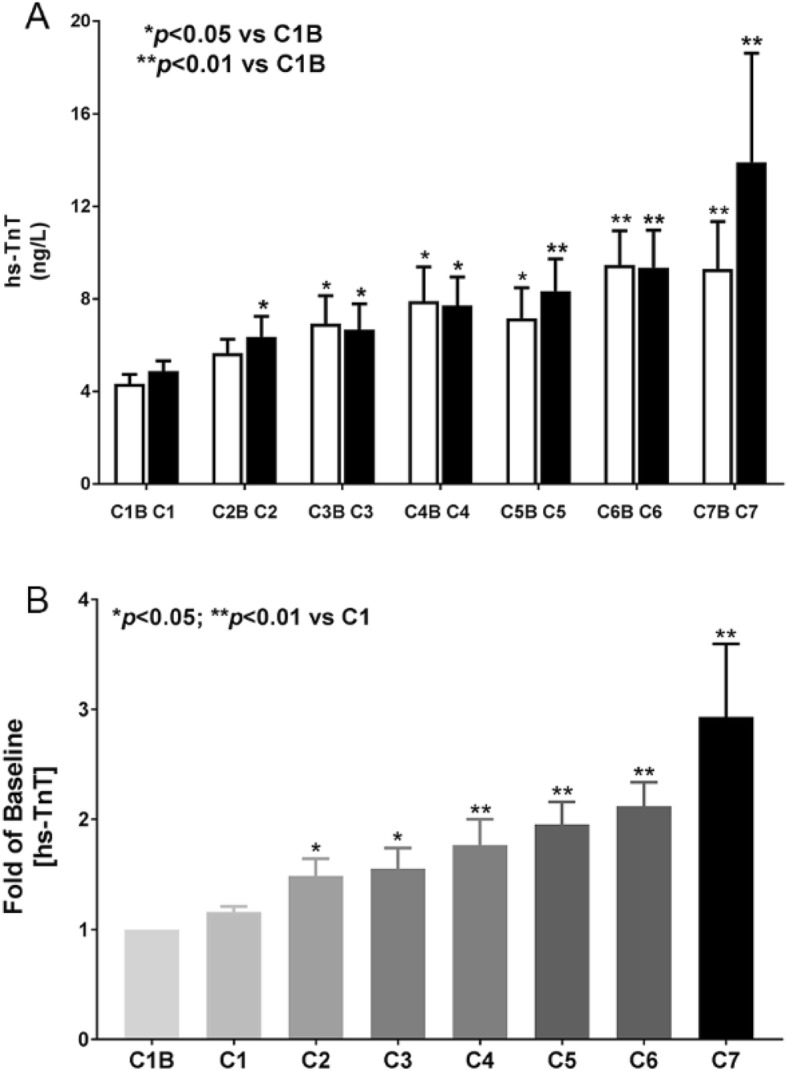
Twenty-nine patients with newly diagnosed sarcoma were assigned to receive either 72-h doxorubicin infusion or dexrazoxane pre-treatment before bolus doxorubicin. Eight patients received dexrazoxane pre-treatment; eleven patients received continuous doxorubicin infusion; ten patients crossed over from continuous infusion to dexrazoxane. Bloods were collected for hs-TnT at baseline, 24 h or 72 h after initiation of doxorubicin treatment in each chemotherapy cycle. All blood samples were assayed in batch using hs-TnT kit from Roche diagnostics. 2D Echo and STE were performed before doxorubicin, after cycle 3, and at the end of chemotherapy.
Seven patients in the cross-over group have at least one hs-TnT measurement between 5 ng/L to 10 ng/L during and after chemotherapy. Ten patients have at least one hs-TnT measurement above 10 ng/ml during and after chemotherapy (six in dexrazoxane group, three in continuous infusion group, one in cross-over group). The average hs-TnT level increases with each additional cycle of doxorubicin treatment. Eight patients had a more than 5% reduction in LVEF at the end of chemotherapy (four in dexrazoxane group, three in continuous infusion group, and one in cross-over group). Four out of these eight patients had a change of GLS by more than 15% (three in the dexrazoxane group).
Elevation in hs-TnT levels were observed in more than 59% of patients who had received either continuous doxorubicin infusion or dexrazoxane pre-treatment before bolus doxorubicin. However, changes in LVEF and GLS were less frequently observed. Thus, continuous doxorubicin infusion or dexrazoxane pre-treatment do not completely ameliorate subclinical doxorubicin-induced cardiotoxicity as detected by more sensitive techniques.
持续输注阿霉素或在推注阿霉素前进行右丙亚胺预处理是预防阿霉素诱导的心脏毒性的已证实策略。最近,用斑点追踪超声心动图(STE)测量的整体纵向峰值收缩应变(GLS)和高敏肌钙蛋白T(hs-TnT)已被确认为阿霉素诱导的心脏毒性的敏感指标。在此,我们探讨在接受持续输注阿霉素或先进行右丙亚胺预处理再推注阿霉素治疗的患者中,是否能检测到hs-TnT和/或GLS的变化。
29例新诊断的肉瘤患者被分配接受72小时阿霉素输注或在推注阿霉素前进行右丙亚胺预处理。8例患者接受右丙亚胺预处理;11例患者接受持续阿霉素输注;10例患者从持续输注转为右丙亚胺治疗。在每个化疗周期中,于阿霉素治疗开始后的基线、24小时或72小时采集血样检测hs-TnT。所有血样均使用罗氏诊断公司的hs-TnT试剂盒进行批量检测。在阿霉素治疗前、第3周期后以及化疗结束时进行二维超声心动图和STE检查。
转换组中有7例患者在化疗期间及化疗后至少有一次hs-TnT测量值在5 ng/L至10 ng/L之间。10例患者在化疗期间及化疗后至少有一次hs-TnT测量值高于10 ng/ml(右丙亚胺组6例,持续输注组3例,转换组1例)。hs-TnT的平均水平随阿霉素治疗的每一个额外周期而升高。8例患者在化疗结束时左心室射血分数(LVEF)降低超过5%(右丙亚胺组4例,持续输注组3例,转换组1例)。这8例患者中有4例GLS变化超过15%(右丙亚胺组3例)。
在接受持续阿霉素输注或在推注阿霉素前进行右丙亚胺预处理的患者中,超过59%的患者观察到hs-TnT水平升高。然而,LVEF和GLS的变化较少见。因此,持续阿霉素输注或右丙亚胺预处理并不能完全改善通过更敏感技术检测到的亚临床阿霉素诱导的心脏毒性。