Irani Shayan, Khashab Mouen
Digestive Disease Institute, Virginia Mason Medical Center, Seattle, Washington.
Department of Gastroenterology, Johns Hopkins University, Baltimore, Maryland, USA.
VideoGIE. 2020 Mar 3;5(3):125-128. doi: 10.1016/j.vgie.2019.12.005. eCollection 2020 Mar.
Certain situations preclude an endoscopic gastroenterostomy (EUS-GE) or enteral stent placement in gastric outlet obstruction (GOO), leaving patients with the option of a surgical bypass or enteral nutrition beyond the point of obstruction. We present a third option in these situations: an endoscopic duodenojejunostomy (EUS-DJ) or jejunojejunostomy (EUS-JJ).
This was a retrospective review of 5 patients whose anatomy precluded an endoscopic gastrojejunostomy and an enteral stent, who underwent a successful EUS-DJ or EUS-JJ from 2016 to 2018.
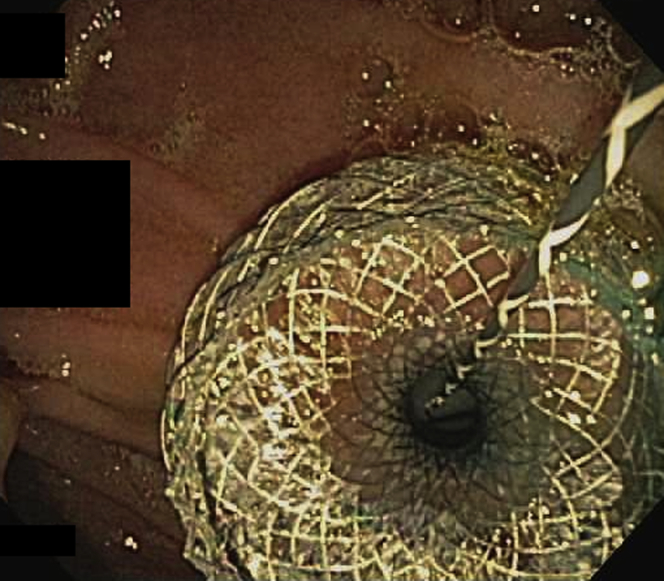
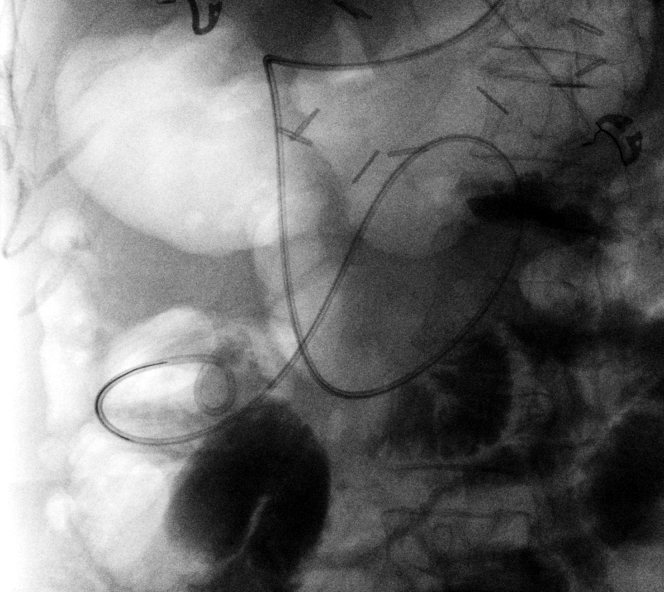
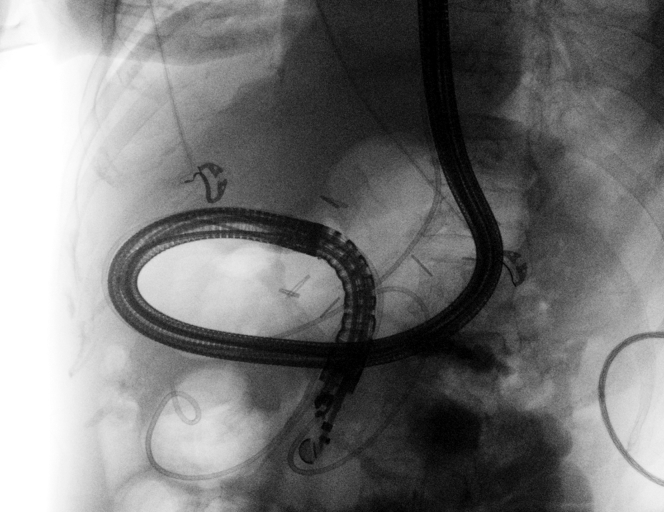
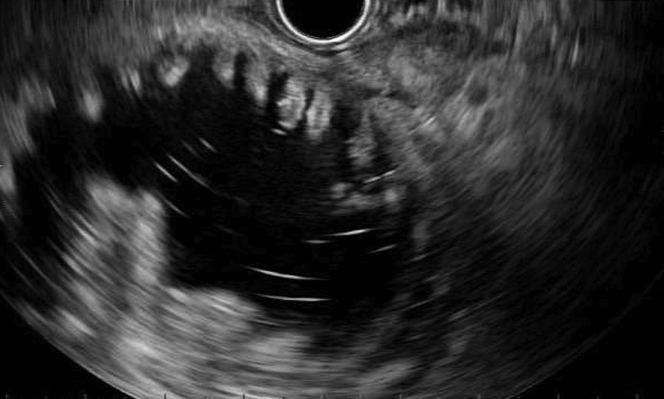
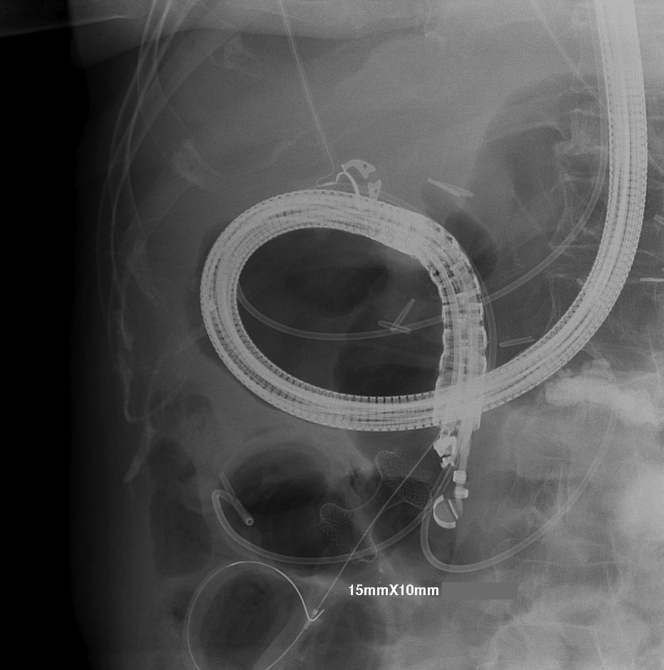
Four EUS-DJs and 1 EUS-JJ were performed, with use of a 15-mm cautery-enhanced lumen-apposing metal stent by direct technique. All cases were technically successful. Three patients tolerated an unrestricted diet, but 2 patients needed enteral supplementation or total parenteral nutrition because of severe gastroparesis. There was 1 moderate adverse event: bleeding from severe reflux esophagitis and gastroparesis. No reinterventions were needed on any of these stents, for a median follow-up time of 23 weeks.
When anatomy precludes an EUS-GE or enteral stent, an EUS-DJ or EUS-JJ may have similarly successful outcomes and could help avoid the need for enteral feeding tubes or surgery.
在某些情况下,内镜下胃肠吻合术(EUS-GE)或肠内支架置入术无法用于治疗胃出口梗阻(GOO),患者只能选择手术旁路或在梗阻部位以外进行肠内营养。在这些情况下,我们提出了第三种选择:内镜下十二指肠空肠吻合术(EUS-DJ)或空肠空肠吻合术(EUS-JJ)。
对2016年至2018年期间接受成功的EUS-DJ或EUS-JJ治疗的5例患者进行回顾性研究,这些患者的解剖结构不适合进行内镜下胃空肠吻合术和肠内支架置入术。
共进行了4例EUS-DJ和1例EUS-JJ,采用直接技术使用15毫米带烧灼增强的管腔贴附金属支架。所有病例技术上均获成功。3例患者能耐受无限制饮食,但2例患者因严重胃轻瘫需要肠内补充营养或全胃肠外营养。发生1例中度不良事件:严重反流性食管炎和胃轻瘫导致出血。这些支架均无需再次干预,中位随访时间为23周。
当解剖结构不适合进行EUS-GE或肠内支架置入时,EUS-DJ或EUS-JJ可能会取得同样成功的结果,并有助于避免使用肠内喂养管或进行手术。