Department of Cardiology II - Electrophysiology, University Hospital Muenster, Cardiol, Muenster, Germany.
Department of Cardiology I - Coronary and Peripheral Vascular Disease, Heart Failure, University Hospital Muenster, Cardiol, Muenster, Germany.
Clin Res Cardiol. 2020 Oct;109(10):1282-1291. doi: 10.1007/s00392-020-01622-z. Epub 2020 Mar 10.
Outcome of ischemic VT ablation may differ between patients with previous myocardial infarction (MI) in relation to infarct localization.
We analyzed procedural data, acute and long-term outcomes of 152 consecutive patients (139 men, mean age 67 ± 9 years) with previous anterior or inferior MI who underwent ischemic VT ablation at our institution between January 2010 and October 2015.
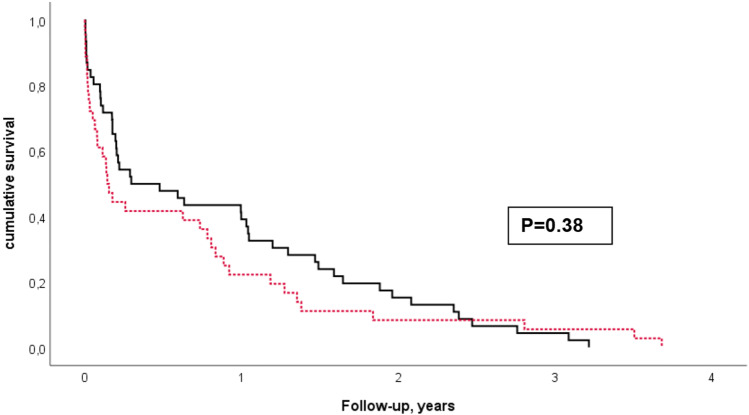
More patients had a history of inferior MI (58%). Mean ejection fraction was significantly lower in anterior MI patients (28 ± 10% vs. 34 ± 10%, p < 0.001). NYHA class and presence of comorbidities were not different between the groups. Indication for the procedure was electrical storm in 43% of patients, and frequent implantable cardioverter defibrillator (ICD) therapies in 57%, and did not differ significantly between anterior and inferior MI patients. A mean of 3 ± 2 VT morphologies were inducible, with a trend towards more VT in the anterior MI group (3.1 ± 2.2 vs. 2.6 ± 1.9, p = 0.18). Procedural parameters and acute success did not differ between the groups. During a mean follow-up of 3 ± 2 years, more anterior MI patients had undergone a re-ablation (49% vs. 33%, p = 0.09, Chi-square test). There was a trend towards more ICD shocks in patients with previous anterior MI (46% vs. 34%). After adjusting for risk factors and ejection fraction, multivariable Cox regression analyses showed no significant difference in mortality (p = 0.78) and cardiovascular mortality between infarct localizations (p = 0.6).
Clinical characteristics of patients with anterior and inferior MI are similar except for ejection fraction. Patients with inferior MI appear to have better outcome regarding survival, ICD shocks and re-ablation, but this appears to be related to better ejection fraction when compared with anterior MI.
缺血性 VT 消融的结果可能因既往心肌梗死(MI)与梗死部位的关系而有所不同。
我们分析了 2010 年 1 月至 2015 年 10 月期间在我院接受缺血性 VT 消融的 152 例连续患者(男 139 例,平均年龄 67 ± 9 岁)的程序数据、急性和长期结果,这些患者既往有前壁或下壁 MI。
更多的患者有下壁 MI 病史(58%)。前壁 MI 患者的平均射血分数显著降低(28 ± 10% vs. 34 ± 10%,p < 0.001)。两组间 NYHA 分级和合并症的存在无差异。电风暴在 43%的患者中是进行该手术的指征,57%的患者是频繁的植入式心脏复律除颤器(ICD)治疗,在这方面,两组间无显著差异。平均可诱发出 3±2 种 VT 形态,前壁 MI 组 VT 更多,呈趋势性(3.1±2.2 vs. 2.6±1.9,p = 0.18)。两组间的程序参数和急性成功率无差异。在平均 3±2 年的随访期间,更多的前壁 MI 患者需要再次消融(49% vs. 33%,p = 0.09,卡方检验)。既往前壁 MI 患者 ICD 电击次数有增加趋势(46% vs. 34%)。调整危险因素和射血分数后,多变量 Cox 回归分析显示,在死亡率(p = 0.78)和梗死部位的心血管死亡率(p = 0.6)方面,无显著差异。
除射血分数外,前壁和下壁 MI 患者的临床特征相似。下壁 MI 患者在生存、ICD 电击和再次消融方面的预后似乎更好,但与前壁 MI 相比,这似乎与射血分数较高有关。