Ruparel Mamta, Quaife Samantha L, Dickson Jennifer L, Horst Carolyn, Tisi Sophie, Hall Helen, Taylor Magali N, Ahmed Asia, Shaw Penny J, Burke Stephen, Soo May-Jan, Nair Arjun, Devaraj Anand, Sennett Karen, Hurst John R, Duffy Stephen W, Navani Neal, Bhowmik Angshu, Baldwin David R, Janes Sam M
Lungs for Living Research Centre, University College London (UCL) Respiratory.
Research Department of Behavioural Science and Health.
Ann Am Thorac Soc. 2020 Jul;17(7):869-878. doi: 10.1513/AnnalsATS.201911-857OC.
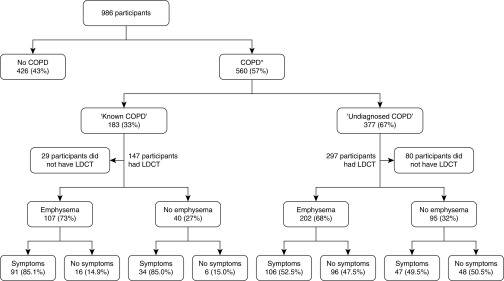
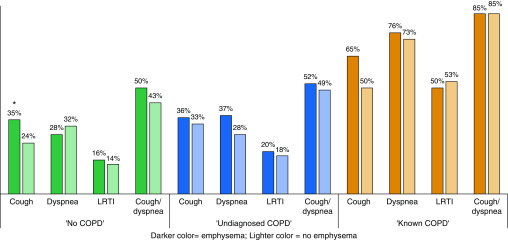
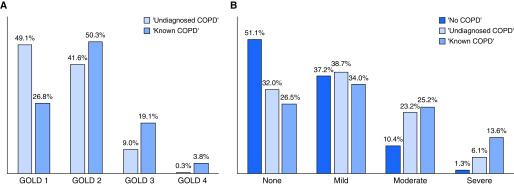
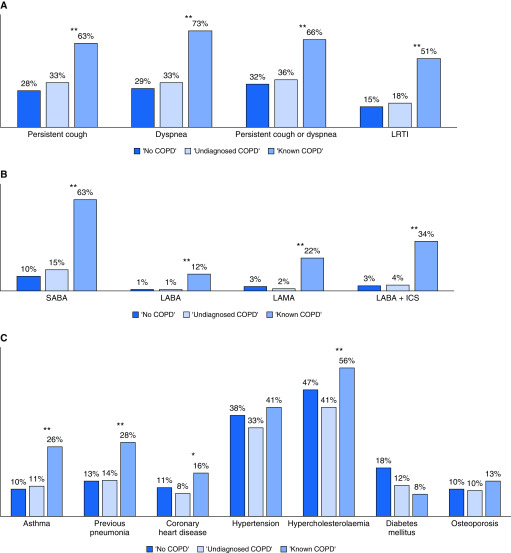
Individuals eligible for lung cancer screening (LCS) by low-dose computed tomography (LDCT) are also at risk of chronic obstructive pulmonary disease (COPD) due to age and smoking exposure. Whether the LCS episode is useful for early detection of COPD is not well established. To explore associations between symptoms, comorbidities, spirometry, and emphysema in participants enrolled in the Lung Screen Uptake Trial. This cross-sectional study was a prespecified analysis nested within Lung Screen Uptake Trial, which was a randomized study testing the impact of differing invitation materials on attendance of 60- to 75-year-old smokers and ex-smokers to a "lung health check" between November 2015 and July 2017. Participants with a smoking history ≥30 pack-years and who quit ≤15 years ago, or meeting a lung cancer risk of ≥1.51% via the Prostate Lung Colorectal Ovarian model or ≥2.5% via the Liverpool Lung Project model, were offered LDCT. COPD was defined and classified according to the GOLD (Global Initiative for Obstructive Lung Disease) criteria using prebronchodilator spirometry. Analyses included the use of descriptive statistics, chi-square tests to examine group differences, and univariable and multivariable logistic regression to explore associations between symptom prevalence, airflow limitation, and visually graded emphysema. A total of 560 of 986 individuals included in the analysis (57%) had prebronchodilator spirometry consistent with COPD; 67% did not have a prior history of COPD and were termed "undiagnosed." Emphysema prevalence in those with known and "undiagnosed" COPD was 73% and 68%, respectively. A total of 32% of those with "undiagnosed COPD" had no emphysema on LDCT. Inhaler use and symptoms were more common in the "known" than the "undiagnosed" COPD group (63% vs. 33% with persistent cough [ < 0.001]; 73% vs. 33% with dyspnea [ < 0.001]). Comorbidities were common in all groups. Adjusted odds ratio (aOR) of respiratory symptoms were more significant for airflow obstruction (aOR GOLD 1 and 2, 1.57; confidence interval [CI], 1.14-2.17; aOR GOLD 3 and 4, 4.6; CI, 2.17-9.77) than emphysema (aOR mild, 1.12; CI, 0.81-1.55; aOR moderate, 1.33; CI, 0.85-2.09; aOR severe, 4.00; CI, 1.57-10.2). There is high burden of "undiagnosed COPD" and emphysema in LCS participants. Adding spirometry findings to the LDCT enhances identification of individuals with COPD.Clinical trial registered with www.clinicaltrials.gov (NCT02558101).
由于年龄和吸烟暴露,符合低剂量计算机断层扫描(LDCT)肺癌筛查(LCS)条件的个体也有患慢性阻塞性肺疾病(COPD)的风险。LCS检查是否有助于COPD的早期检测尚未明确。旨在探讨参加肺癌筛查接受试验的参与者的症状、合并症、肺功能测定和肺气肿之间的关联。这项横断面研究是肺癌筛查接受试验中的一项预先设定的分析,肺癌筛查接受试验是一项随机研究,测试了2015年11月至2017年7月期间不同邀请材料对60至75岁吸烟者和戒烟者参加“肺部健康检查”的影响。吸烟史≥30包年且在≤15年前戒烟的参与者,或通过前列腺、肺癌、结直肠癌、卵巢癌模型肺癌风险≥1.51%或通过利物浦肺癌项目模型肺癌风险≥2.5%的参与者,接受LDCT检查。根据全球阻塞性肺疾病倡议(GOLD)标准,使用支气管扩张剂前肺功能测定对COPD进行定义和分类。分析包括使用描述性统计、卡方检验以检查组间差异,以及单变量和多变量逻辑回归以探索症状患病率、气流受限和视觉分级肺气肿之间的关联。分析纳入的986名个体中,共有560名(57%)支气管扩张剂前肺功能测定结果符合COPD;67%没有COPD病史,被称为“未确诊”。已知COPD和“未确诊”COPD患者的肺气肿患病率分别为73%和68%。“未确诊COPD”患者中共有32%在LDCT上没有肺气肿。吸入器使用和症状在“已知”COPD组比“未确诊”COPD组更常见(持续性咳嗽分别为63%对33%[<0.001];呼吸困难分别为73%对33%[<0.001])。合并症在所有组中都很常见。呼吸症状的调整优势比(aOR)在气流阻塞方面比肺气肿更显著(GOLD 1和2级,aOR为1.57;置信区间[CI],1.14 - 2.17;GOLD 3和4级,aOR为4.6;CI,2.17 - 9.77)(轻度肺气肿,aOR为1.12;CI,0.81 - 1.55;中度肺气肿,aOR为1.33;CI,0.85 - 2.09;重度肺气肿,aOR为4.00;CI,1.57 - 10.2)。LCS参与者中“未确诊COPD”和肺气肿的负担很高。将肺功能测定结果添加到LDCT中可增强对COPD个体的识别。在www.clinicaltrials.gov注册的临床试验(NCT02558101)。