BHF Centre for Cardiovascular Science, University of Edinburgh, Room SU.305 Chancellor's Building, Edinburgh, EH16 4SB, UK.
Geriatric Medicine Research Group, University of Edinburgh, Edinburgh, UK.
BMC Geriatr. 2020 Mar 13;20(1):102. doi: 10.1186/s12877-020-1500-9.
Risk prediction after myocardial infarction is often complex in older patients. The Global Registry of Acute Coronary Events (GRACE) model includes clinical parameters and age, but not frailty. We hypothesised that frailty would enhance the prognostic properties of GRACE.
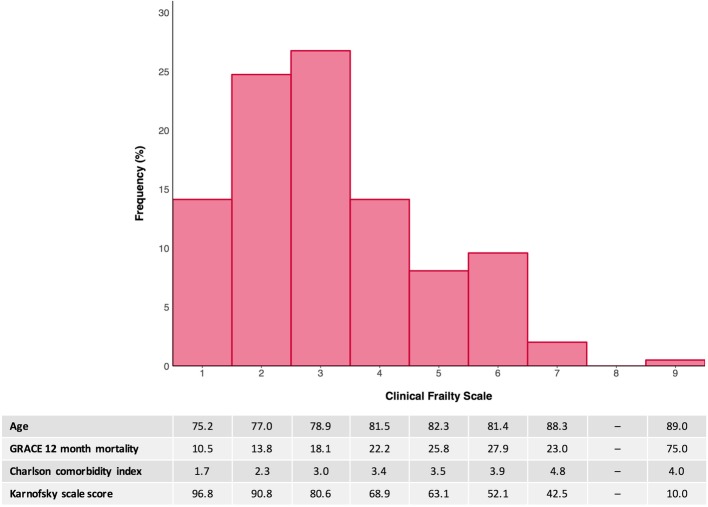
We performed a prospective observational cohort study in two independent cardiology units: the Royal Infirmary of Edinburgh, UK (primary cohort) and the South Yorkshire Cardiothoracic Centre, Sheffield, UK (external validation). The study sample included 198 patients ≥65 years old hospitalised with type 1 myocardial infarction (primary cohort) and 96 patients ≥65 years old undergoing cardiac catheterisation for myocardial infarction (external validation). Frailty was assessed using the Clinical Frailty Scale (CFS). The GRACE 2.0 estimated risk of 12-month mortality, Charlson comorbidity index and Karnofsky disability scale were also determined for each patient.
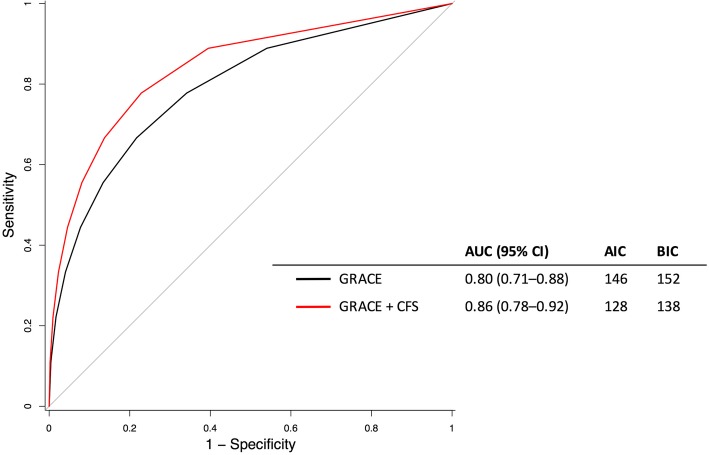
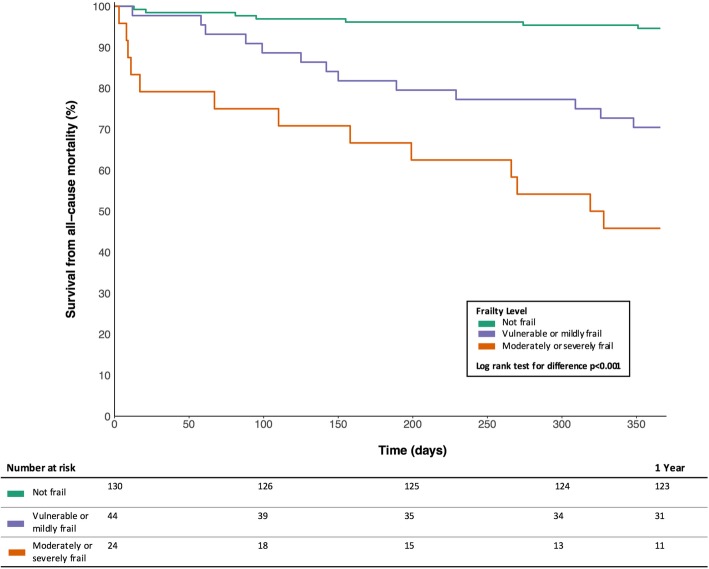
Forty (20%) patients were frail (CFS ≥5). These individuals had greater comorbidity, functional impairment and a higher risk of death at 12 months (49% vs. 9% in non-frail patients, p < 0.001). The hazard of 12-month all-cause mortality nearly doubled per point increase in CFS after adjustment for age, sex and comorbidity (Hazard Ratio [HR] 1.90, 95% CI 1.47-2.44, p < 0.001). The CFS had good discrimination for mortality by Receiver Operating Characteristic (ROC) curve analysis (Area Under the Curve [AUC] 0.81, 95% CI 0.72-0.89) and enhanced the GRACE estimate (AUC 0.86 vs. 0.80 without CFS, p = 0.04). At existing GRACE thresholds, the CFS resulted in a Net Reclassification Improvement (NRI) of 0.44 (95% CI 0.28-0.60, p < 0.001), largely through reductions in risk estimates amongst non-frail patients. Similar findings were observed in the external validation cohort (NRI 0.46, 95% CI 0.23-0.69, p < 0.001).
The GRACE score overestimated mortality risk after myocardial infarction in these cohorts of older patients. The CFS is a simple guided frailty tool that may enhance prediction in this setting. These findings merit evaluation in larger cohorts of unselected patients.
Clinicaltrials.gov; NCT02302014 (November 26th 2014, retrospectively registered).
心肌梗死后的风险预测在老年患者中通常较为复杂。全球急性冠状动脉事件注册(GRACE)模型包含临床参数和年龄,但不包括虚弱。我们假设虚弱会增强 GRACE 的预后性能。
我们在两个独立的心脏病学单位进行了前瞻性观察队列研究:英国爱丁堡皇家医院(主要队列)和英国谢菲尔德南约克郡心胸中心(外部验证)。研究样本包括 198 名年龄≥65 岁的因 1 型心肌梗死住院的患者(主要队列)和 96 名年龄≥65 岁因心肌梗死行心导管检查的患者(外部验证)。使用临床虚弱量表(CFS)评估虚弱。还为每位患者确定了 GRACE 2.0 估计的 12 个月死亡率、Charlson 合并症指数和卡诺夫斯基残疾量表。
40 名(20%)患者为虚弱状态(CFS≥5)。这些患者的合并症更多、功能障碍更严重,12 个月时死亡风险更高(49%比非虚弱患者的 9%,p<0.001)。在调整年龄、性别和合并症后,CFS 每增加 1 分,12 个月全因死亡率的危险比(HR)增加近 1 倍(HR 1.90,95%置信区间 1.47-2.44,p<0.001)。CFS 通过接收者操作特征(ROC)曲线分析对死亡率具有良好的区分度(曲线下面积[AUC] 0.81,95%置信区间 0.72-0.89),并增强了 GRACE 估计值(AUC 0.86 与无 CFS 时的 0.80,p=0.04)。在现有的 GRACE 阈值下,CFS 导致净重新分类改善(NRI)为 0.44(95%置信区间 0.28-0.60,p<0.001),主要是通过降低非虚弱患者的风险估计值。在外部验证队列中也观察到类似的发现(NRI 0.46,95%置信区间 0.23-0.69,p<0.001)。
在这些老年患者队列中,GRACE 评分高估了心肌梗死后的死亡率风险。CFS 是一种简单的衰弱指导工具,可在该环境中增强预测能力。这些发现值得在更大的未选择患者队列中进行评估。
Clinicaltrials.gov;NCT02302014(2014 年 11 月 26 日,回顾性注册)。