Nanna Michael G, Sutton Nadia R, Kochar Ajar, Rymer Jennifer A, Lowenstern Angela M, Gackenbach Grace, Hummel Scott L, Goyal Parag, Rich Michael W, Kirkpatrick James N, Krishnaswami Ashok, Alexander Karen P, Forman Daniel E, Bortnick Anna E, Batchelor Wayne, Damluji Abdulla A
Yale University School of Medicine, New Haven, Connecticut, USA.
Department of Internal Medicine, Division of Cardiovascular Medicine, Michigan Medicine, Ann Arbor, Michigan, USA.
JACC Adv. 2023 Jun;2(4). doi: 10.1016/j.jacadv.2023.100389.
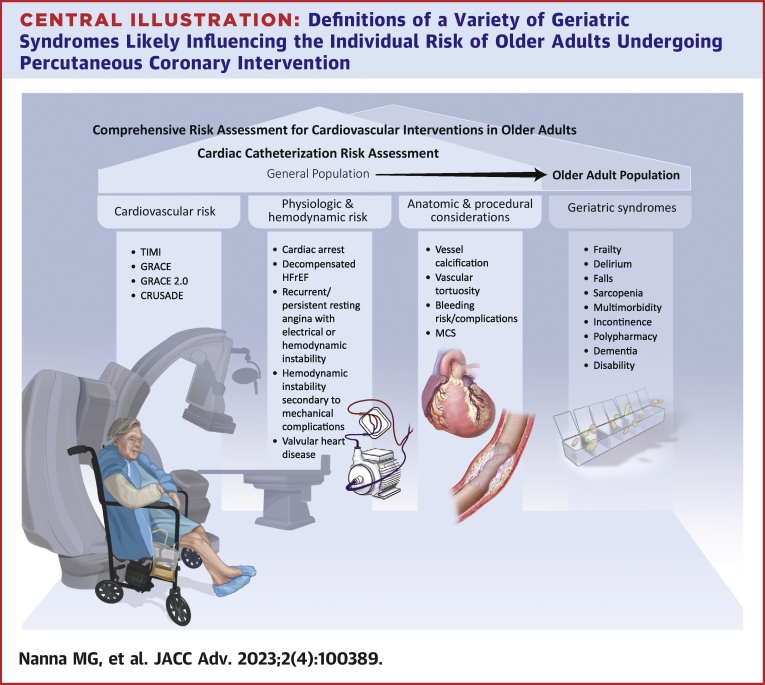
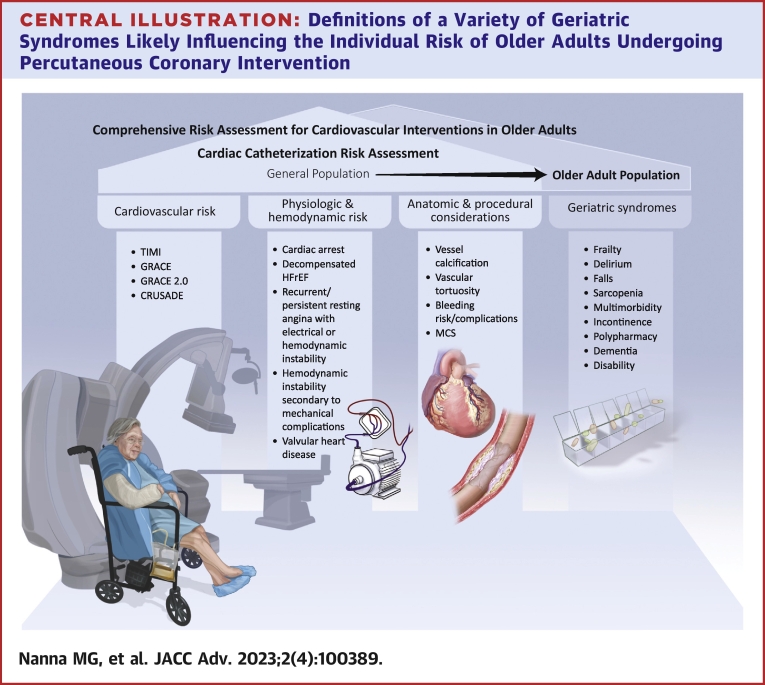
As the population ages, older adults represent an increasing proportion of patients referred to the cardiac catheterization laboratory. Older adults are the highest-risk group for morbidity and mortality, particularly after complex, high-risk percutaneous coronary interventions. Structured risk assessment plays a key role in differentiating patients who are likely to derive net benefit vs those who have disproportionate risks for harm. Conventional risk assessment tools from national cardiovascular societies typically rely on 3 pillars: 1) cardiovascular risk; 2) physiologic and hemodynamic risk; and 3) anatomic and procedural risks. We propose adding a fourth pillar: geriatric syndromes, as geriatric domains can supersede all other aspects of risk.
随着人口老龄化,老年人在被转诊至心导管实验室的患者中所占比例越来越大。老年人是发病和死亡风险最高的群体,尤其是在进行复杂、高风险的经皮冠状动脉介入治疗之后。结构化风险评估在区分可能获得净收益的患者与那些面临不成比例伤害风险的患者方面起着关键作用。国家心血管学会的传统风险评估工具通常依赖三个支柱:1)心血管风险;2)生理和血流动力学风险;3)解剖和手术风险。我们建议增加第四个支柱:老年综合征,因为老年领域可以超越风险的所有其他方面。