Ahoua Laurence, Arikawa Shino, Tiendrebeogo Thierry, Lahuerta Maria, Aly Dario, Becquet Renaud, Dabis Francois
University of Bordeaux, INSERM, Bordeaux Population Health Research Center, Team IDLIC, UMR 1219, Université de Bordeaux, Case 11, 146 rue Léo Saignat, 33076, Bordeaux Cedex, France.
Mailman School of Public Health, ICAP at Columbia University, Rua Francisco Matange, 224/246, Caixa Postal n.°1747, Maputo, Mozambique.
BMC Public Health. 2020 Mar 12;20(1):322. doi: 10.1186/s12889-020-8406-5.
Failure to retain HIV-positive pregnant women on antiretroviral therapy (ART) leads to increased mortality for the mother and her child. This study evaluated different retention measures for women's engagement along the continuum of care for prevention of mother-to-child transmission (PMTCT) option B+ services in Mozambique.
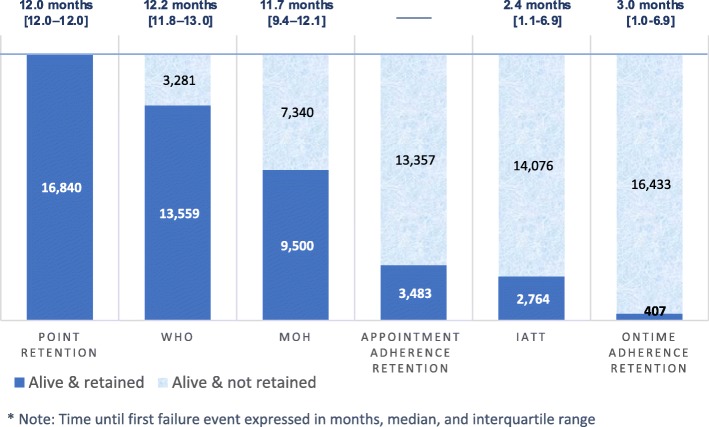
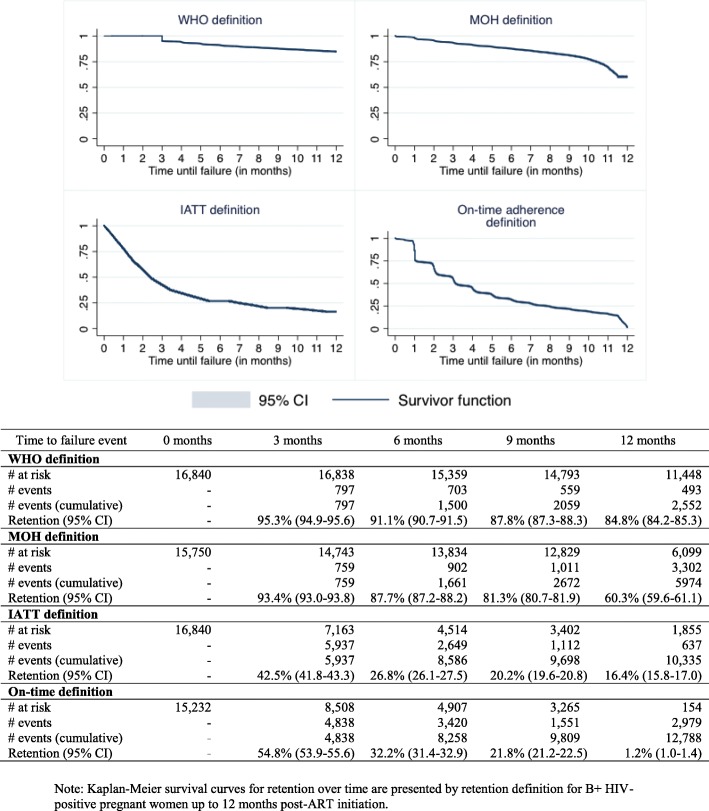
We compared 'point' retention (patient's presence in care 12-month post-ART initiation or any time thereafter) with the following definitions: alive and in care 12 month post-ART initiation (Ministry of Health; MOH); attendance at a health facility up to 15-month post-ART initiation (World Health Organization; WHO); alive and in treatment at 1-, 2-, 3-, 6-, 9-, and 12-month post-ART initiation (Inter-Agency Task Team; IATT); and alive and in care 12-month post-ART initiation with ≥75% appointment adherence during follow-up (i.e. 'appointment adherence' retention) or with ≥75% of appointments met on time during follow-up (i.e. 'on-time adherence' retention). Kaplan-Meier survival curves were produced to assess variability in retention rates. We used 'on-time adherence' retention as our reference to estimate sensitivity, specificity, and proportion of misclassified patients.
Considering the 'point' retention definition, 16,840 HIV-positive pregnant women enrolled in option B+ PMTCT services were identified as 'retained in care' 12-month post-ART initiation. Of these, 60.3% (95% CI 59.6-61.1), 84.8% (95% CI 84.2-85.3), and 16.4% (95% CI 15.8-17.0) were classified as 'retained in care' using MOH, WHO, and IATT definitions, respectively, and 1.2% (95% CI 1.0-1.4) were classified as 'retained in care' using the '≥75% on-time adherence' definition. All definitions provided specificity rates of ≥98%. The sensitivity rates were 3.0% with 78% of patients misclassified according to the WHO definition and 4.3% with 54% of patients misclassified according to the MOH definition. The 'point' retention definition misclassified 97.6% of patients. Using IATT and 'appointment adherence' retention definitions, sensitivity rates (9.0 and 11.7%, respectively) were also low; however, the proportion of misclassified patients was smaller (15.9 and 18.3%, respectively).
More stringent definitions indicated lower retention rates for PMTCT programs. Policy makers and program managers should include attendance at follow-up visits when measuring retention in care to better guide planning, scale-up, and monitoring of interventions.
未能使感染艾滋病毒的孕妇坚持接受抗逆转录病毒治疗(ART)会导致母亲及其子女的死亡率上升。本研究评估了莫桑比克为预防母婴传播(PMTCT)B+方案提供的连续性护理中,针对女性参与情况的不同留存措施。
我们将“定点”留存(ART开始后12个月或之后任何时间患者接受护理的情况)与以下定义进行比较:ART开始后12个月存活且接受护理(卫生部;MOH);ART开始后15个月内到医疗机构就诊(世界卫生组织;WHO);ART开始后1、2、3、6、9和12个月存活且接受治疗(机构间特别工作组;IATT);以及ART开始后12个月存活且接受护理,随访期间预约依从率≥75%(即“预约依从性”留存)或随访期间≥75%的预约按时完成(即“按时依从性”留存)。绘制Kaplan-Meier生存曲线以评估留存率的变异性。我们以“按时依从性”留存作为参考来估计敏感度、特异度和分类错误患者的比例。
考虑“定点”留存定义,16840名登记参加B+ PMTCT服务的艾滋病毒阳性孕妇在ART开始后12个月被确定为“留存于护理中”。其中,分别使用MOH、WHO和IATT定义时,60.3%(95%CI 59.6 - 61.1)、84.8%(95%CI 84.2 - 85.3)和16.4%(95%CI 15.8 - 17.0)被分类为“留存于护理中”,使用“≥75%按时依从性”定义时,1.2%(95%CI 1.0 - 1.4)被分类为“留存于护理中”。所有定义的特异度率均≥98%。根据WHO定义,敏感度率为3.0%,78%的患者分类错误;根据MOH定义,敏感度率为4.3%,54%的患者分类错误。“定点”留存定义将97.6%的患者分类错误。使用IATT和“预约依从性”留存定义时,敏感度率也较低(分别为9.0%和11.7%);然而,分类错误患者的比例较小(分别为15.9%和18.3%)。
更严格的定义表明PMTCT项目的留存率较低。政策制定者和项目管理者在衡量护理留存情况时应将随访就诊纳入考量,以更好地指导干预措施的规划、扩大规模和监测。