Centre for Prevention of Stroke and Dementia, University of Oxford, Oxford, Oxfordshire, UK.
Centre for Prevention of Stroke and Dementia, University of Oxford, Oxford, Oxfordshire, UK
J Neurol Neurosurg Psychiatry. 2020 Jun;91(6):580-585. doi: 10.1136/jnnp-2019-322663. Epub 2020 Mar 12.
Patients with primary intracerebral haemorrhage (ICH) are at increased long-term risks of recurrent stroke and other comorbidities. However, available estimates come predominantly from hospital-based studies with relatively short follow-up. Moreover, there are also uncertainties about the influence of ICH location on risks of recurrent stroke, disability, dementia and quality of life.
In a population-based study (Oxford Vascular Study/2002-2018) of patients with a first ICH with follow-up to 10 years, we determined the long-term risks of recurrent stroke, disability, quality of life, dementia and hospital care costs stratified by haematoma location.
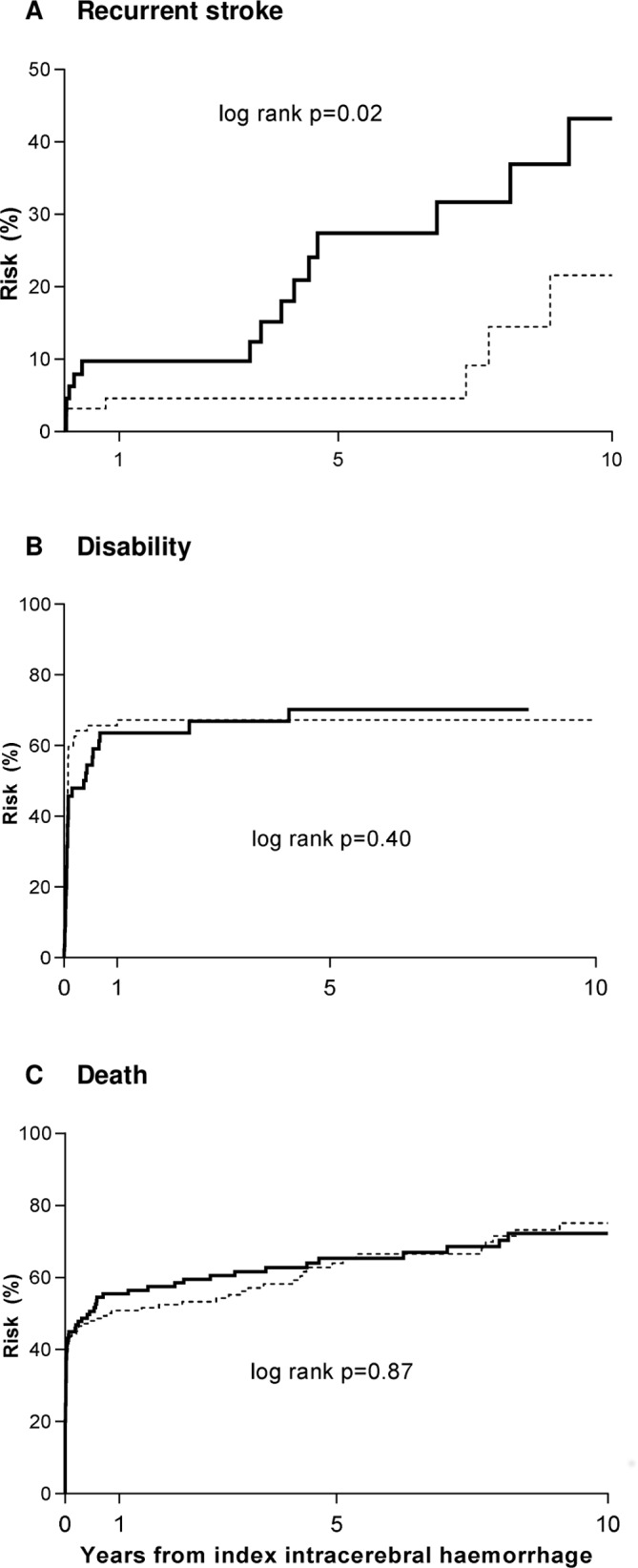
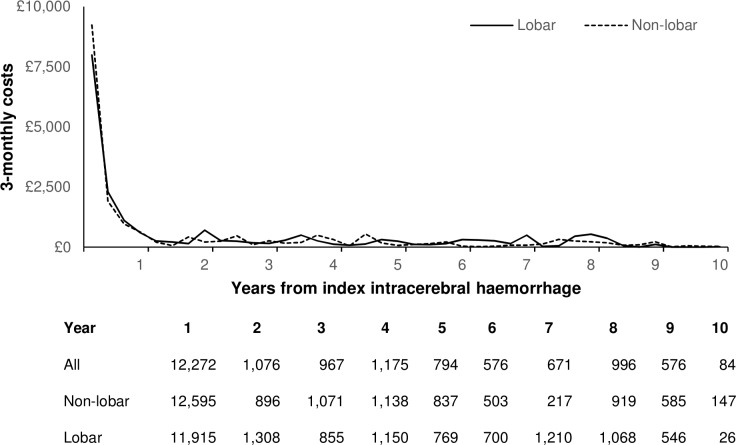
Of 255 cases with primary ICH (mean/SD age 75.5/13.1), 109 (42.7%) had lobar ICH, 144 (56.5%) non-lobar ICH and 2 (0.8%) had uncertain location. Annual rates of recurrent ICH were higher after lobar versus non-lobar ICH (lobar=4.0%, 2.7-7.2 vs 1.1%, 0.3-2.8; p=0.02). Moreover, cumulative rate of dementia was also higher for lobar versus non-lobar ICH (n/% lobar=20/36.4% vs 16/20.8%, p=0.047), and there was a higher proportion of disability at 5 years in survivors (15/60.0% vs 9/31.0%, p=0.03). The 10-year quality-adjusted life years (QALYs) were also lower after lobar versus non-lobar ICH (2.9 vs 3.8 for non-lobar, p=0.04). Overall, the mean 10-year censor-adjusted costs were £19 292, with over 80% of costs due to inpatient hospital admission costs, which did not vary by haematoma location (p=0.90).
Compared with non-lobar ICH, the substantially higher 10-year risks of recurrent stroke, dementia and lower QALYs after lobar ICH highlight the need for more effective prevention for this patient group.
原发性脑出血(ICH)患者长期存在复发性中风和其他合并症的风险增加。然而,现有评估主要来自于随访时间相对较短的基于医院的研究。此外,ICH 位置对复发性中风、残疾、痴呆和生活质量风险的影响也存在不确定性。
在一项基于人群的研究(牛津血管研究/2002-2018 年)中,我们对首次 ICH 患者进行了长达 10 年的随访,根据血肿位置对复发性中风、残疾、生活质量、痴呆和住院护理费用的长期风险进行了分层。
在 255 例原发性 ICH 患者中(平均/标准差年龄 75.5/13.1),109 例(42.7%)为皮质下ICH,144 例(56.5%)为非皮质下 ICH,2 例(0.8%)为位置不确定。皮质下 ICH 后复发性 ICH 的年发生率高于非皮质下 ICH(皮质下=4.0%,2.7-7.2% vs 1.1%,0.3-2.8%;p=0.02)。此外,皮质下 ICH 的痴呆累积发生率也高于非皮质下 ICH(皮质下 20/36.4%,非皮质下 16/20.8%,p=0.047),且幸存者在 5 年内残疾比例更高(皮质下 15/60.0%,非皮质下 9/31.0%,p=0.03)。皮质下 ICH 后的 10 年质量调整生命年(QALYs)也低于非皮质下 ICH(皮质下 2.9,非皮质下 3.8,p=0.04)。总体而言,10 年平均 censored-adjusted 成本为 19292 英镑,其中超过 80%的成本归因于住院治疗费用,这与血肿位置无关(p=0.90)。
与非皮质下 ICH 相比,皮质下 ICH 后 10 年复发性中风、痴呆风险显著增加,QALYs 降低,这突出表明需要为这一患者群体制定更有效的预防措施。