Crowley Conor P, Logiudice Rebecca E, Salciccioli Justin D, McCannon Jessica B, Clardy Peter F
Critical Care Department, Mount Auburn Hospital, Cambridge, MA.
Critical Care Department, North Shore Medical Center, Salem, MA.
Crit Care Explor. 2020 Jan 29;2(1):e0069. doi: 10.1097/CCE.0000000000000069. eCollection 2020 Jan.
Compliance to advanced cardiac life support algorithm is low and associated with worse outcomes from in-hospital cardiac arrests. This study aims to improve algorithm compliance by delegation of two separate code team members for timing rhythm check and epinephrine administration in accordance to the advanced cardiac life support algorithm.
Prospective intervention with historical controls.
Single academic medical center.
Patients who suffered in-hospital cardiac arrest during study period were considered for inclusion. Patients in which the advanced cardiac life support algorithm or new timekeeper roles were not used were excluded.
Two existing code team members were delegated to time epinephrine and rhythm checks.
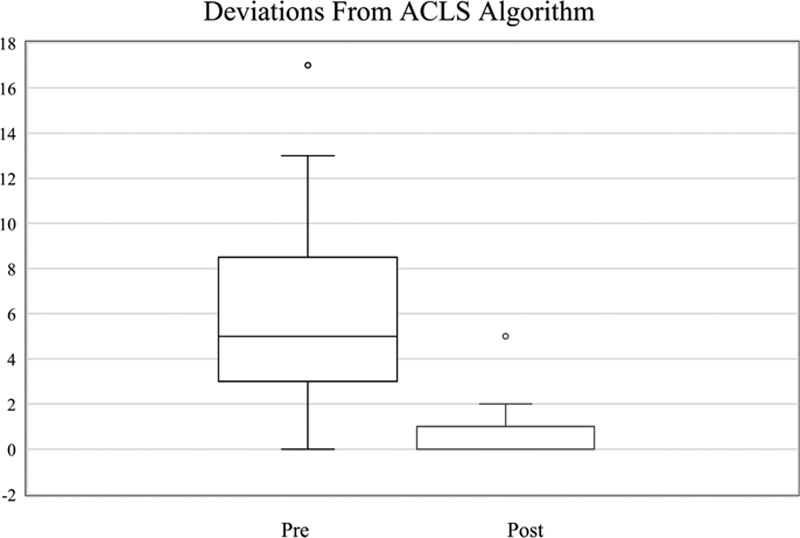
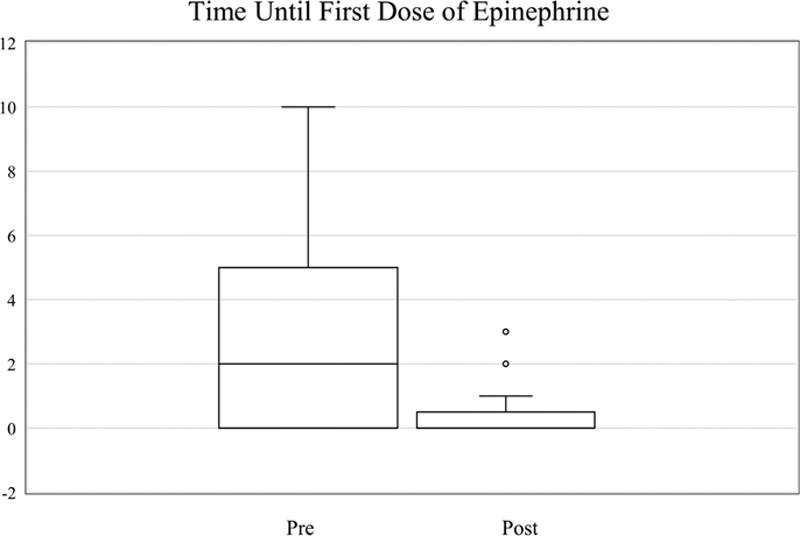
Primary endpoint was deviations from the 2-minute rhythm check or 3- to 5-minute epinephrine administration. Each deviation outside allotted time intervals was counted as one deviation. However, instances in which multiple intervals passed were counted as multiple deviations. Algorithm adherence was analyzed before and after intervention. Secondary endpoints included return of spontaneous circulation rate, time until first dose of epinephrine, and anonymous survey data. Thirteen pre intervention in-hospital cardiac arrests were compared with 13 in-hospital cardiac arrests post. Prior to intervention, the median deviation per in-hospital cardiac arrest was 5 (interquartile range, 3-7) versus 1 post (interquartile range 0-1; = 0.0003). The median time until first dose of epinephrine was administered pre intervention was 5 minutes (interquartile range, 0-4) versus post intervention median of 0 (interquartile range, 0-0; = 0.02). Pre-intervention return of spontaneous circulation rate was 46.1% versus 69.2% post. Surveys demonstrated advanced cardiac life support providers felt time keeping roles made it easier to track epinephrine administration and rhythm checks and improved team communication.
Two separate timekeeper roles during in-hospital cardiac arrests improved algorithm compliance, code team function, and was favored by code team members. Timekeeper roles may be associated with improved rates of return of spontaneous circulation and less time until the first dose of epinephrine was administered. This study is limited by small sample size and single-center design.
高级心脏生命支持算法的依从性较低,且与院内心脏骤停的较差预后相关。本研究旨在通过根据高级心脏生命支持算法委派两名独立的急救团队成员分别进行心律检查计时和肾上腺素给药,来提高算法依从性。
采用历史对照的前瞻性干预研究。
单一学术医疗中心。
研究期间发生院内心脏骤停的患者被纳入研究。未使用高级心脏生命支持算法或新计时员角色的患者被排除。
委派两名现有的急救团队成员分别对肾上腺素给药和心律检查进行计时。
主要终点为偏离2分钟心律检查或3至5分钟肾上腺素给药的情况。每个超出规定时间间隔的偏差计为一次偏差。然而,多个时间间隔过去的情况计为多次偏差。分析干预前后的算法依从性。次要终点包括自主循环恢复率、首次给予肾上腺素的时间以及匿名调查数据。将13例干预前的院内心脏骤停与13例干预后的院内心脏骤停进行比较。干预前,每次院内心脏骤停的中位偏差为5(四分位间距,3 - 7),而干预后为1(四分位间距0 - 1;P = 0.0003)。干预前首次给予肾上腺素的中位时间为5分钟(四分位间距,0 - 4),而干预后中位时间为0(四分位间距,0 - 0;P = 0.02)。干预前自主循环恢复率为46.1%,干预后为69.2%。调查显示,高级心脏生命支持提供者认为计时员角色使跟踪肾上腺素给药和心律检查更容易,并改善了团队沟通。
院内心脏骤停期间设立两个独立的计时员角色可提高算法依从性、急救团队功能,并受到急救团队成员的青睐。计时员角色可能与更高的自主循环恢复率以及首次给予肾上腺素的时间缩短有关。本研究受样本量小和单中心设计的限制。