Doyle Andrew J, Richardson Carla, Sanderson Barnaby, Wong Katie, Wyncoll Duncan, Camporota Luigi, Barrett Nicholas A, Hunt Beverley J, Retter Andrew
Department of Haematology, Guy's & St Thomas NHS Foundation Trust, London, United Kingdom.
Department of Intensive Care, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham, Birmingham, United Kingdom.
Crit Care Explor. 2020 Jan 29;2(1):e0077. doi: 10.1097/CCE.0000000000000077. eCollection 2020 Jan.
Restrictive transfusion policies have been adopted in critical care, although these have not included patients receiving extracorporeal membrane oxygenation. We aimed to assess survival outcomes, adverse events related to RBC transfusion, and cost implications following a change from a "liberal" to a "restrictive" RBC transfusion practice in patients receiving extracorporeal membrane oxygenation.
Retrospective observational study.
Single high-volume tertiary critical care department at a university hospital.
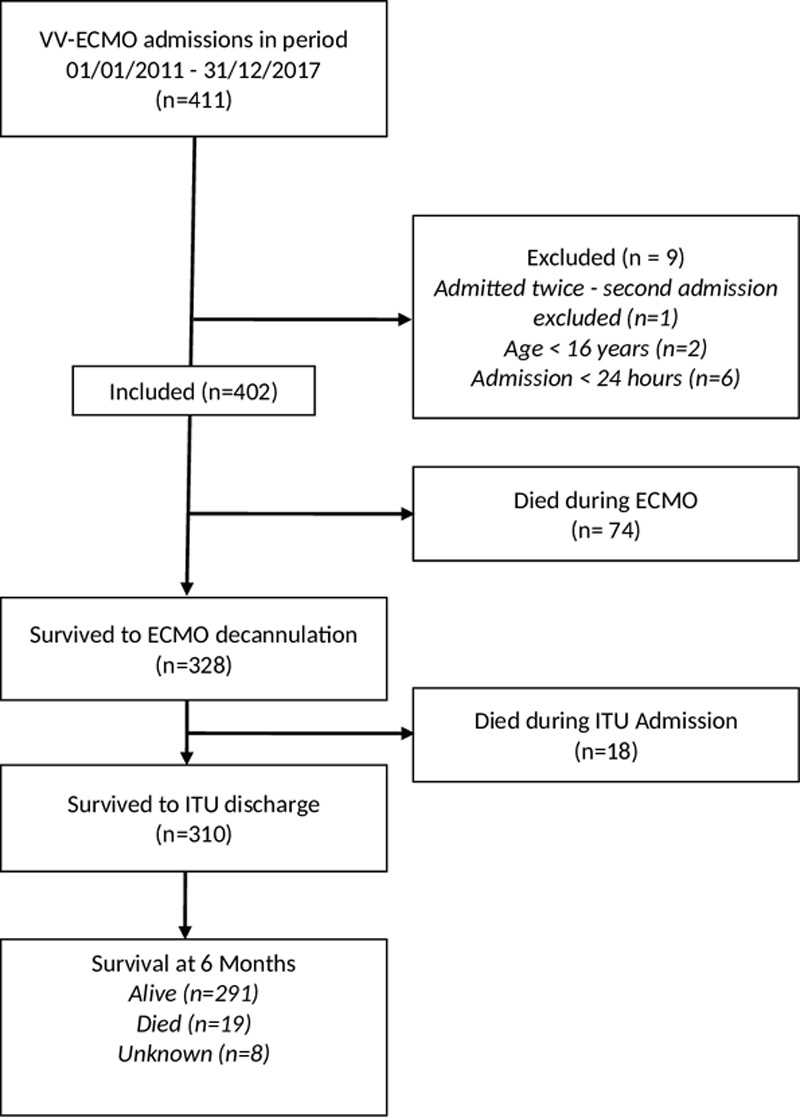
Patients 16 years old or greater receiving venovenous extracorporeal membrane oxygenation between 2011 and 2017 for more than 24 hours.
None.
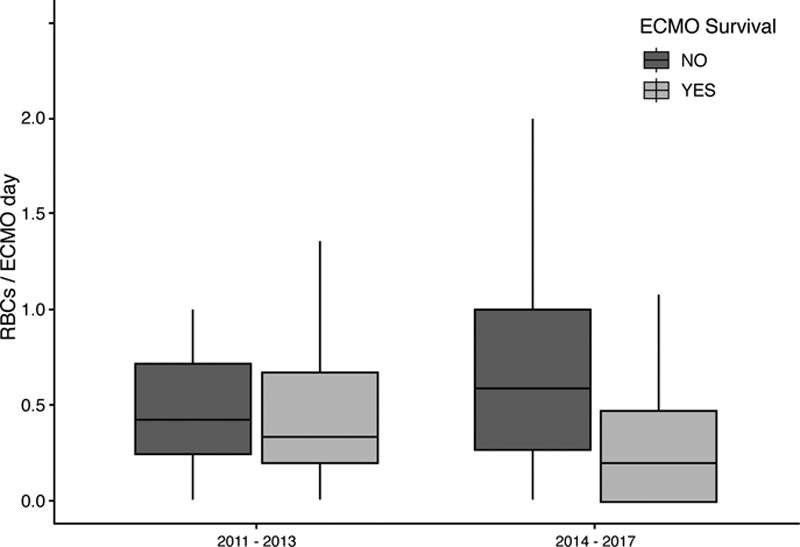
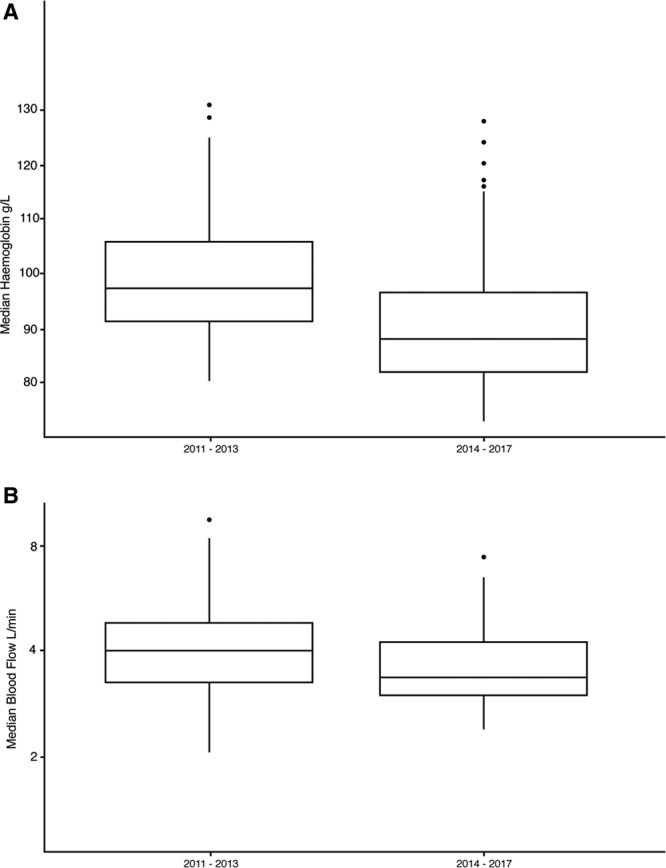
Clinical diagnoses, complications, outcomes, median hemoglobin, and hematocrit levels were obtained from patients' electronic records. All laboratory results for hemoglobin and hematocrit were included. RBC transfusions were obtained from prescription charts. We included 402 patients: 99 during a "liberal" transfusion practice (2011-2014)-when the target hemoglobin level was greater than 100 g/L; and 303 treated during a "restrictive" transfusion practice (2014-2017) when the target hemoglobin level was greater than 80 g/L. We found that survival outcomes did not change following the implementation of a "restrictive" transfusion policy. There was also a decrease in the extracorporeal blood flow rates with restrictive transfusion of 0.5 L/min. Nonsurvivors of venovenous extracorporeal membrane oxygenation had higher usage of RBC units following a change in transfusion practice. The restrictive strategy allowed a cost saving of £454 per patient.
These results suggest that the adoption of a more restrictive approach to RBC transfusion during venovenous extracorporeal membrane oxygenation is more cost-effective and associated with similar survival outcomes, than when compared with a more liberal approach.
尽管重症监护中已采用限制性输血策略,但这些策略并未涵盖接受体外膜肺氧合(ECMO)的患者。我们旨在评估接受ECMO的患者从“宽松”的红细胞(RBC)输血策略转变为“限制性”输血策略后的生存结局、与RBC输血相关的不良事件以及成本影响。
回顾性观察研究。
一所大学医院的单一高容量三级重症监护科室。
2011年至2017年间接受静脉-静脉ECMO治疗超过24小时的16岁及以上患者。
无。
从患者电子记录中获取临床诊断、并发症、结局、血红蛋白中位数和血细胞比容水平。纳入所有血红蛋白和血细胞比容的实验室结果。从处方图表中获取RBC输血情况。我们纳入了402例患者:99例在“宽松”输血策略实施期间(2011 - 2014年),此时目标血红蛋白水平大于100 g/L;303例在“限制性”输血策略实施期间(2014 - 2017年)接受治疗,此时目标血红蛋白水平大于80 g/L。我们发现实施“限制性”输血策略后生存结局未发生变化。限制性输血时体外血流量速率也降低了0.5 L/min。静脉-静脉ECMO的非幸存者在输血策略改变后RBC单位使用量更高。限制性策略使每位患者节省成本454英镑。
这些结果表明,与更宽松的方法相比,在静脉-静脉ECMO期间采用更具限制性的RBC输血方法更具成本效益,且生存结局相似。