Section for Experimental Neuropsychiatry, Department of Psychiatry and Psychotherapy, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
Department of Psychiatry and Psychotherapy, Medical Center - University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
Eur Arch Psychiatry Clin Neurosci. 2020 Oct;270(7):803-818. doi: 10.1007/s00406-020-01113-2. Epub 2020 Mar 12.
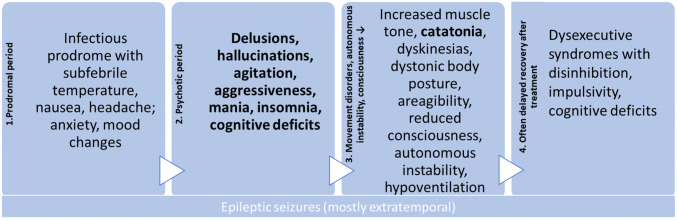
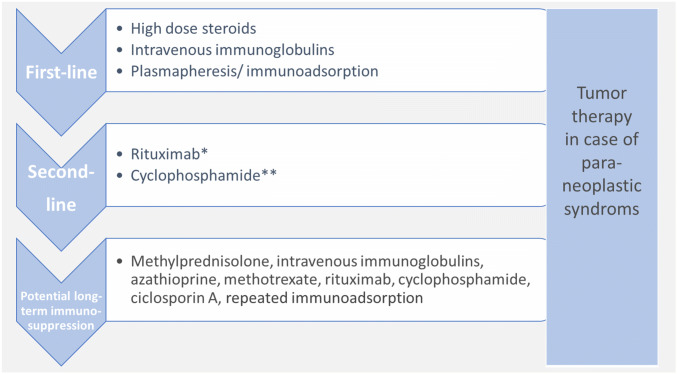
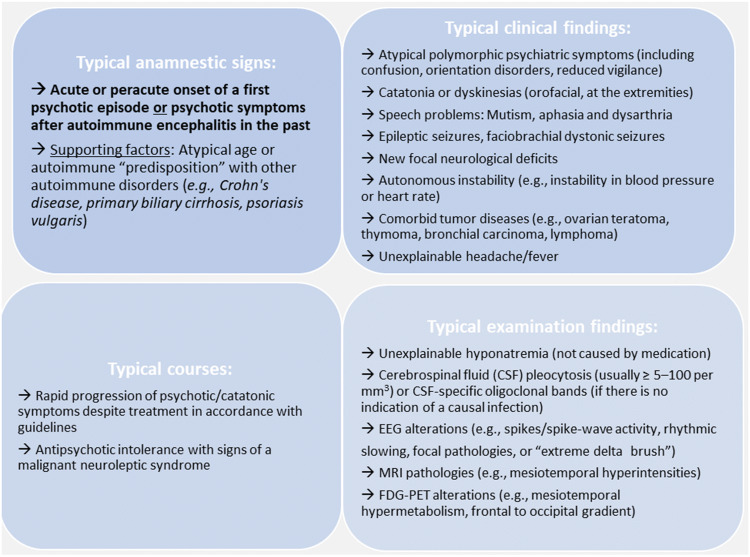
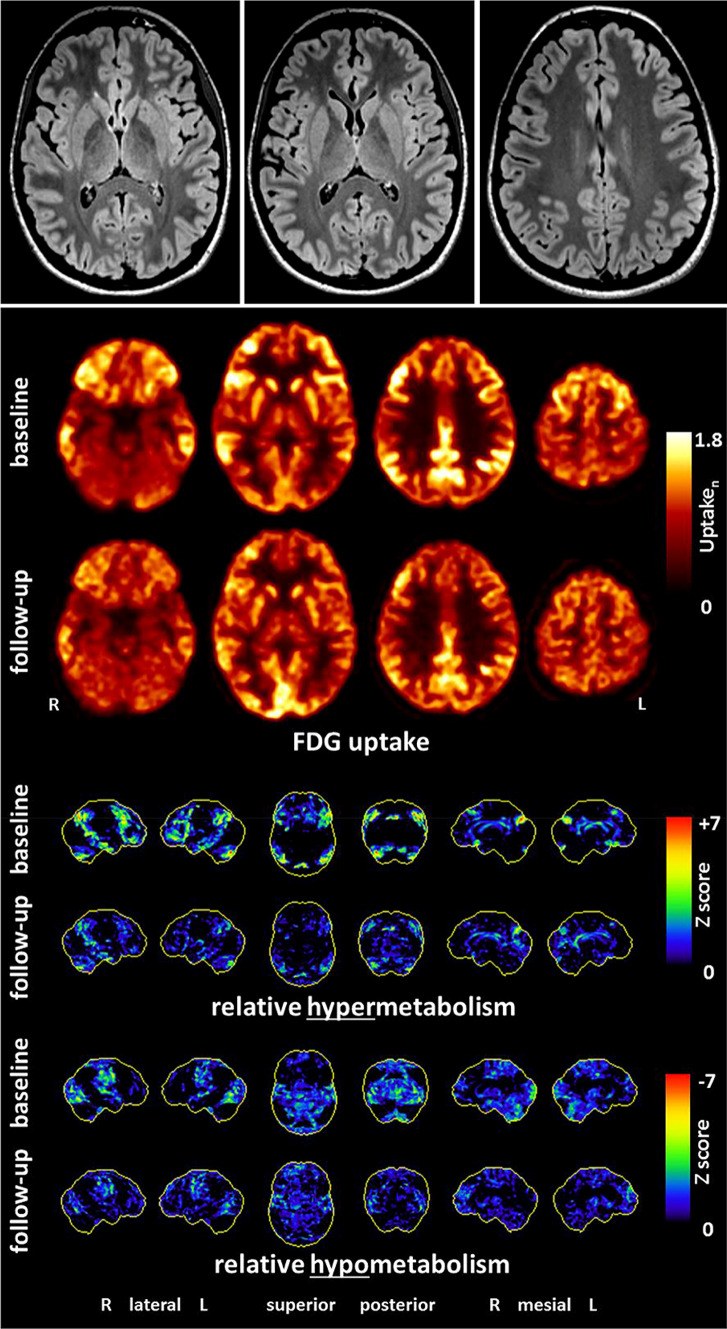
Primary schizophreniform psychoses are thought to be caused by complex gene-environment interactions. Secondary forms are based on a clearly identifiable organic cause, in terms of either an etiological or a relevant pathogenetic factor. The secondary or "symptomatic" forms of psychosis have reentered the focus stimulated by the discovery of autoantibody (Ab)-associated autoimmune encephalitides (AEs), such as anti-NMDA-R encephalitis, which can at least initially mimic variants of primary psychosis. These newly described secondary, immune-mediated schizophreniform psychoses typically present with the acute onset of polymorphic psychotic symptoms. Over the course of the disease, other neurological phenomena, such as epileptic seizures, movement disorders, or reduced levels of consciousness, usually arise. Typical clinical signs for AEs are the acute onset of paranoid hallucinatory symptoms, atypical polymorphic presentation, psychotic episodes in the context of previous AE, and additional neurological and medical symptoms such as catatonia, seizure, dyskinesia, and autonomic instability. Predominant psychotic courses of AEs have also been described casuistically. The term autoimmune psychosis (AP) was recently suggested for these patients. Paraclinical alterations that can be observed in patients with AE/AP are inflammatory cerebrospinal fluid (CSF) pathologies, focal or generalized electroencephalographic slowing or epileptic activity, and/or suspicious "encephalitic" imaging findings. The antibody analyses in these patients include the testing of the most frequently found Abs against cell surface antigens (NMDA-R, CASPR2, LGI1, AMPA-R, GABA-R), intracellular antigens (Hu, Ri, Yo, CV2/CRMP5, Ma2 [Ta], amphiphysin, GAD65), thyroid antigens (TG, TPO), and antinuclear Abs (ANA). Less frequent antineuronal Abs (e.g., against DPPX, GABA-R, glycine-R, IgLON5) can be investigated in the second step when first step screening is negative and/or some specific clinical factors prevail. Beyond, tissue-based assays on brain slices of rodents may detect previously unknown antineuronal Abs in some cases. The detection of clinical and/or paraclinical pathologies (e.g., pleocytosis in CSF) in combination with antineuronal Abs and the exclusion of alternative causes may lead to the diagnosis of AE/AP and enable more causal therapeutic immunomodulatory opportunities.
原发性分裂型精神病被认为是由复杂的基因-环境相互作用引起的。继发性形式基于明确可识别的器质性原因,无论是病因学还是相关的发病机制因素。继发性或“症状性”精神病形式在自身抗体 (Ab) 相关自身免疫性脑炎 (AE) 的发现所激发的关注下重新进入焦点,例如抗 NMDA-R 脑炎,它至少最初可以模拟原发性精神病的变体。这些新描述的继发性、免疫介导的分裂型精神病通常以多形性精神病症状的急性发作为特征。在疾病过程中,通常会出现其他神经现象,例如癫痫发作、运动障碍或意识水平降低。AE 的典型临床体征是偏执幻觉症状的急性发作、非典型多形性表现、AE 背景下的精神病发作以及其他神经和医学症状,如紧张症、癫痫发作、运动障碍和自主神经不稳定。AE 也有描述过占主导地位的精神病病程。最近提出了自身免疫性精神病 (AP) 这个术语来描述这些患者。AE/AP 患者可观察到的副临床改变包括炎症性脑脊液 (CSF) 病理学、局灶性或全身性脑电图减慢或癫痫活动,以及/或可疑的“脑炎样”影像学发现。这些患者的抗体分析包括最常发现的针对细胞表面抗原 (NMDA-R、CASPR2、LGI1、AMPA-R、GABA-R)、细胞内抗原 (Hu、Ri、Yo、CV2/CRMP5、Ma2 [Ta]、 amphiphysin、GAD65)、甲状腺抗原 (TG、TPO) 和抗核抗体 (ANA) 的检测。当第一步筛选呈阴性且/或存在一些特定的临床因素时,可以在第二步检测较少见的神经元抗体(例如,针对 DPPX、GABA-R、glycine-R、IgLON5)。此外,在某些情况下,啮齿动物脑组织切片上的基于组织的检测可能会检测到以前未知的神经元抗体。临床和/或副临床病理的检测(例如 CSF 中的白细胞增多)与神经元抗体相结合,并排除其他原因,可能导致 AE/AP 的诊断,并提供更多因果治疗免疫调节机会。