National Clinical Research Center for Hematologic Disease, Beijing Key Laboratory of Hematopoietic Stem Cell Transplantation, Peking University People's Hospital, Peking University Institute of Hematology, Beijing, 100044, P. R. China.
Department of Hematology, Xinqiao Hospital, Army Military Medical University, Chongqing, 400037, P. R. China.
Cancer Commun (Lond). 2020 Mar;40(2-3):93-104. doi: 10.1002/cac2.12014. Epub 2020 Mar 16.
Human leukocyte antigen-identical sibling donor (ISD)-hematopoietic stem cell transplantation (SCT) is a potentially curative treatment for high-risk pediatric acute myeloid leukemia (AML). A haploidentical donor (HID) is readily available to almost all children. Previous studies have demonstrated that patients with HID-SCT had similar outcomes compared to ISD-SCT for pediatric and adult AML. However, the role of HID-SCT in high-risk pediatric AML is unclear.
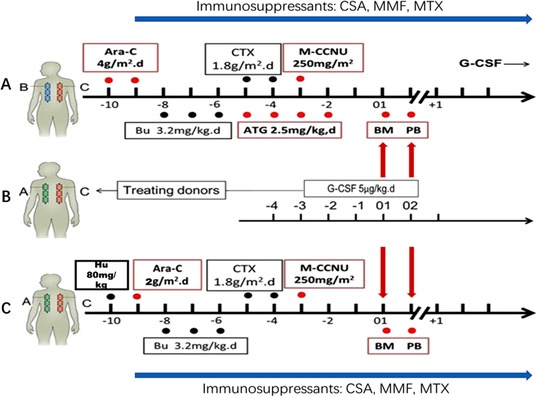
To compare the overall survival of high-risk AML children who underwent either HID-SCT or ISD-SCT, we analyzed 179 cases of high-risk AML patients under 18 years of age treated with either ISD-SCT (n = 23) or HID-SCT (n = 156). Granulocyte colony-stimulating factor plus anti-thymocyte globulin-based regimens were used for HID-SCT. We also analyzed the subgroup data of AML patients at first complete remission (CR1) before SCT with known cytogenetic risk.
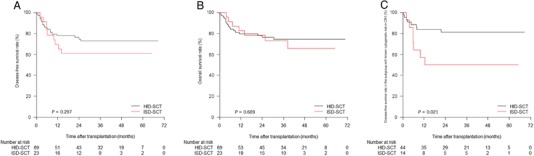
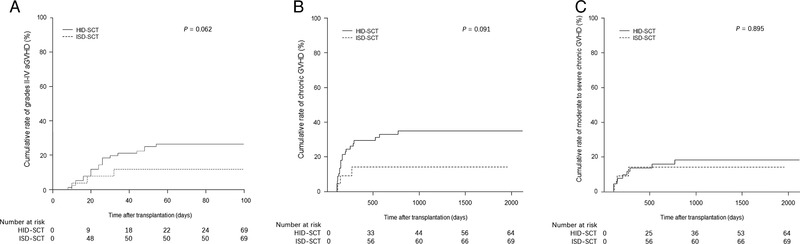
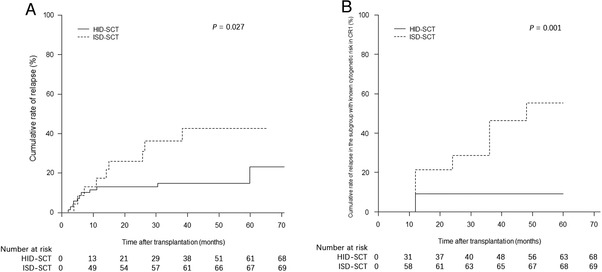
The numbers of adverse cytogenetic risk recipients were 8 (34.8%) and 13 (18.8%) in the ISD-SCT group and the HID-SCT group, and the number of patients with disease status beyond CR1 were 6 (26.1%) and 14 (20.3%) in the two groups. The cumulative rates of grades II-IV acute graft-versus-host disease (GVHD) were 13.0% in the ISD-SCT group and 34.8% in the HID-SCT group (P = 0.062), with a three-year cumulative rates of chronic GVHD at 14.1% and 34.9%, respectively (P = 0.091). The relapse rate in the ISD-SCT group was significantly higher than that in the HID-SCT group (39.1% vs. 16.4%, P = 0.027); with non-relapse mortality at 0.0% and 10.6% (P = 0.113), respectively. The three-year overall survival rates were 73.0% for the ISD-SCT group and 74.6% for the HID-SCT group (P = 0.689). In subgroup analysis, the three-year relapse rate in the ISD-SCT group was higher than that in the HID-SCT group (50.0% vs. 9.2%, P = 0.001) and the three-year DFS in the ISD-SCT group (50.0%) was lower than that in the HID-SCT group (81.2%) (P = 0.021).
Unmanipulated HID-SCT achieved DFS and OS outcomes comparable to those of ISD-SCT for high-risk pediatric AML patients with potentially higher rate but manageable GVHD.
人类白细胞抗原相合同胞供者(ISD)-造血干细胞移植(SCT)是一种有治愈潜力的治疗高危儿科急性髓系白血病(AML)的方法。几乎所有儿童都可以获得单倍体相合供者(HID)。先前的研究表明,HID-SCT 患者与 ISD-SCT 患者在儿科和成人 AML 方面的结局相似。然而,HID-SCT 在高危儿科 AML 中的作用尚不清楚。
为了比较接受 HID-SCT 或 ISD-SCT 的高危 AML 儿童的总体生存率,我们分析了 179 例年龄在 18 岁以下接受 ISD-SCT(n=23)或 HID-SCT(n=156)的高危 AML 患者。采用粒细胞集落刺激因子加抗胸腺细胞球蛋白方案进行 HID-SCT。我们还分析了 SCT 前处于首次完全缓解(CR1)的 AML 患者的亚组数据,这些患者具有已知的细胞遗传学风险。
ISD-SCT 组和 HID-SCT 组中不良细胞遗传学风险受体的数量分别为 8(34.8%)和 13(18.8%),疾病状态超出 CR1 的患者数量分别为 6(26.1%)和 14(20.3%)。ISD-SCT 组中 II-IV 级急性移植物抗宿主病(GVHD)的累积发生率为 13.0%,HID-SCT 组为 34.8%(P=0.062),两组 3 年慢性 GVHD 的累积发生率分别为 14.1%和 34.9%(P=0.091)。ISD-SCT 组的复发率明显高于 HID-SCT 组(39.1% vs. 16.4%,P=0.027),非复发死亡率分别为 0.0%和 10.6%(P=0.113)。ISD-SCT 组的 3 年总生存率为 73.0%,HID-SCT 组为 74.6%(P=0.689)。在亚组分析中,ISD-SCT 组的 3 年复发率高于 HID-SCT 组(50.0% vs. 9.2%,P=0.001),ISD-SCT 组的 3 年无病生存率(DFS)也低于 HID-SCT 组(50.0% vs. 81.2%,P=0.021)。
未经处理的 HID-SCT 为高危儿科 AML 患者带来了与 ISD-SCT 相当的 DFS 和 OS 结局,GVHD 的发生率可能更高,但可管理。