Division of Oncology, Stanford University School of Medicine, Stanford, California.
Medical Services, Veterans Affairs Palo Alto Health Care System, Palo Alto, California.
JAMA Netw Open. 2020 Mar 2;3(3):e201023. doi: 10.1001/jamanetworkopen.2020.1023.
Undertreated patient symptoms require approaches that improve symptom burden.
To determine the association of a lay health worker-led symptom screening and referral intervention with symptom burden, survival, health care use, and total costs among Medicare Advantage enrollees with a new diagnosis of solid or hematologic malignant neoplasms.
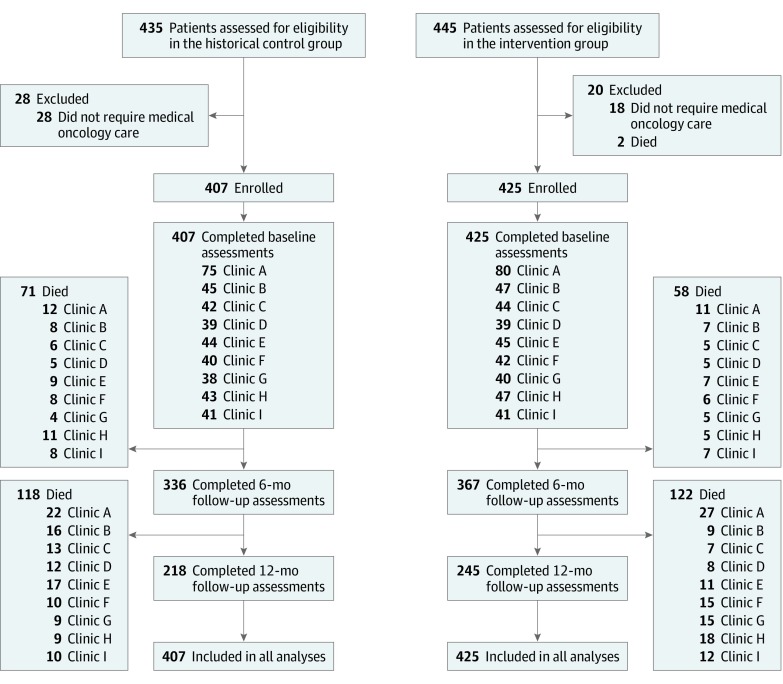
DESIGN, SETTING, AND PARTICIPANTS: This quality improvement study conducted at 9 community oncology practices from November 1, 2016, to October 31, 2018, compared newly diagnosed Medicare Advantage enrollees with solid or hematologic malignant neoplasms with patients diagnosed and treated 1 year prior. Analysis was conducted from August 1, 2019, to January 11, 2020.
Usual care augmented by a lay health worker trained to screen symptoms and refer patients to palliative care and behavioral medicine.
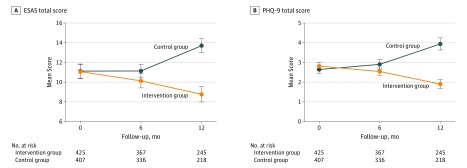
The primary outcome was change in symptoms using the Edmonton Symptom Assessment Scale and the 9-item Patient Health Questionnaire at baseline and 6 and 12 months after enrollment. Secondary outcomes were between-group comparison of survival, 12-month health care use, and costs.
Among 425 patients in the intervention group and 407 patients in the control group, the mean (SD) age was 78.8 (8.3) years, 345 (41.5%) were female, and 407 (48.9%) were non-Hispanic white. Patients in the intervention group experienced a lower symptom burden as measured by the Edmonton Symptom Assessment Scale score over time compared with patients in the control group (mean [SD] difference, -1.9 [14.2]; 95% CI, -3.77 to -0.19; P = .01 for the intervention group and 2.32 [17.7]; 95% CI, 0.47 to 4.19; P = .02 for the control group). Similar findings were noted in 9-item Patient Health Questionnaire depression scores (mean [SD] difference, -0.63 [3.99]; 95% CI, -1.23 to -0.028; P = .04 for the intervention group and 1.67 [5.49]; 95% CI, 0.95 to 2.37; P = .01 for the control group). Patients in the intervention group compared with patients in the control group had fewer mean (SD) inpatient visits (0.54 [0.77]; 95% CI, 0.47-0.61 vs 0.72 [1.12]; 95% CI, 0.61-0.83; P = .04) and emergency department visits (0.43 [0.76]; 95% CI, 0.36-0.50 vs 0.57 [1.00]; 95% CI, 0.48-0.67; P = .002) per 1000 patients per year and lower total costs (median, $17 869 [interquartile range, $6865-$32 540] vs median, $18 473 [interquartile range, $6415-$37 910]; P = .02). A total of 180 patients in the intervention group and 189 patients in the control group died within 12 months. Among those who died, patients in the intervention group had greater hospice use (125 of 180 [69.4%] vs 79 of 189 [41.8%]; odds ratio, 3.16; 95% CI, 2.13-4.69; P < .001), fewer mean (SD) emergency department and hospital visits (emergency department: 0.10 [0.30]; 95% CI, 0.06-0.14 vs 0.30 [0.46]; 95% CI, 0.24-0.38; P = .001; hospital: 0.27 [0.44]; 95% CI, 0.21-0.34 vs 0.43 [0.82]; 95% CI, 0.32-0.55; P = .02), and lower costs (median, $3602 [interquartile range, $1076-$9436] vs median, $12 726 [interquartile range, $5259-$22 170]; P = .002), but there was no significant difference in inpatient deaths (18 of 180 [10.0%] vs 30 of 189 [15.9%]; P = .14).
This study suggests that a lay health worker-led intervention may be one way to improve burdensome and costly care.
未得到充分治疗的患者症状需要采用能改善症状负担的方法。
确定由非专业卫生工作者主导的症状筛查和转介干预措施对新诊断出患有实体或血液恶性肿瘤的医疗保险优势计划参保者的症状负担、生存、医疗保健使用情况和总费用的影响。
设计、设置和参与者:这项质量改进研究于 2016 年 11 月 1 日至 2018 年 10 月 31 日在 9 家社区肿瘤学诊所进行,比较了新诊断出患有实体或血液恶性肿瘤的医疗保险优势计划参保者与 1 年前确诊和治疗的患者。分析于 2019 年 8 月 1 日至 2020 年 1 月 11 日进行。
在常规护理的基础上,增加经过培训的非专业卫生工作者,以筛查症状并将患者转介至姑息治疗和行为医学科。
主要结果是使用埃德蒙顿症状评估量表和 9 项患者健康问卷在基线和入组后 6 个月和 12 个月时评估症状变化。次要结果是生存、12 个月医疗保健使用情况和成本的组间比较。
在干预组的 425 名患者和对照组的 407 名患者中,平均(SD)年龄为 78.8(8.3)岁,345 名(41.5%)为女性,407 名(48.9%)为非西班牙裔白人。与对照组相比,干预组患者的症状负担随着时间的推移呈下降趋势,表现为埃德蒙顿症状评估量表评分降低(平均[SD]差异,-1.9[14.2];95%CI,-3.77 至-0.19;P=0.01;干预组和 2.32[17.7];95%CI,0.47 至 4.19;P=0.02;对照组)。9 项患者健康问卷抑郁评分也出现了类似的结果(平均[SD]差异,-0.63[3.99];95%CI,-1.23 至-0.028;P=0.04;干预组和 1.67[5.49];95%CI,0.95 至 2.37;P=0.01;对照组)。与对照组相比,干预组患者的平均(SD)住院就诊次数(0.54[0.77];95%CI,0.47 至 0.61 与 0.72[1.12];95%CI,0.61 至 0.83;P=0.04)和急诊就诊次数(0.43[0.76];95%CI,0.36 至 0.50 与 0.57[1.00];95%CI,0.48 至 0.67;P=0.002)更少,总费用更低(中位数,17869 美元[四分位距,6865 美元至 32540 美元]与中位数,18473 美元[四分位距,6415 美元至 37910 美元];P=0.02)。干预组中有 180 名患者和对照组中有 189 名患者在 12 个月内死亡。在死亡的患者中,干预组患者的临终关怀使用率更高(180 名中的 125 名[69.4%]与 189 名中的 79 名[41.8%];比值比,3.16;95%CI,2.13 至 4.69;P<0.001),急诊和住院就诊次数更少(急诊就诊:0.10[0.30];95%CI,0.06 至 0.14 与 0.30[0.46];95%CI,0.24 至 0.38;P=0.001;住院就诊:0.27[0.44];95%CI,0.21 至 0.34 与 0.43[0.82];95%CI,0.32 至 0.55;P=0.02),成本更低(中位数,3602 美元[四分位距,1076 美元至 9436 美元]与中位数,12726 美元[四分位距,5259 美元至 22170 美元];P=0.002),但住院死亡无显著差异(180 名中的 18 名[10.0%]与 189 名中的 30 名[15.9%];P=0.14)。
本研究表明,由非专业卫生工作者主导的干预措施可能是改善负担沉重和昂贵的护理的一种方法。