Singh Rashmi, Garg Mandeep, Sodhi Kushaljit S, Prabhakar Nidhi, Singh Paramjeet, Agarwal Ritesh, Malhotra Pankaj
Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Pol J Radiol. 2020 Jan 29;85:e53-e61. doi: 10.5114/pjr.2020.93258. eCollection 2020.
To evaluate the accuracy of magnetic resonance imaging (MRI) for diagnosing pulmonary infections in immunocompromised adults.
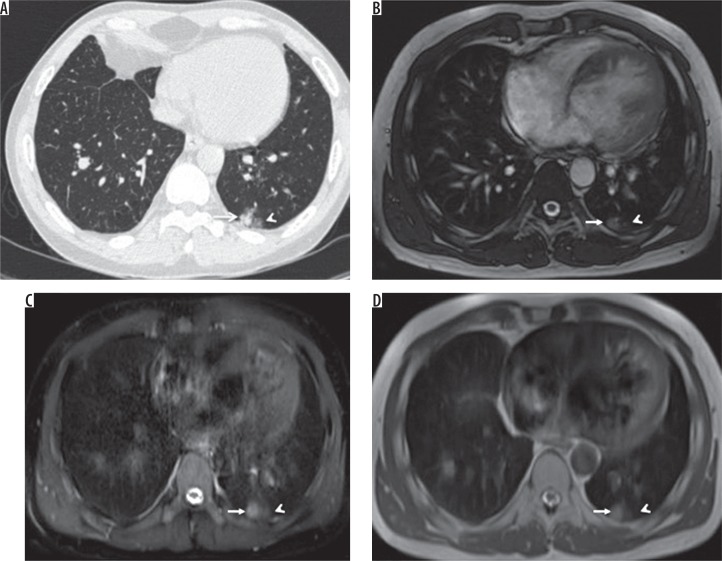
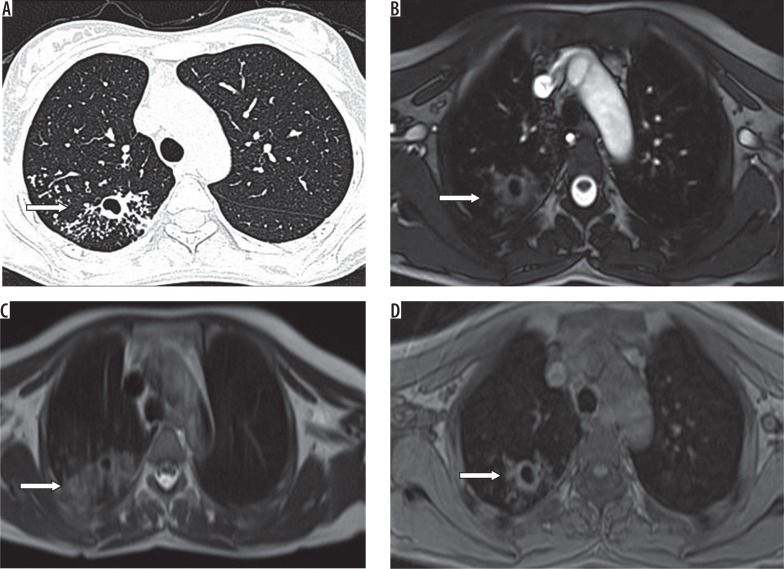
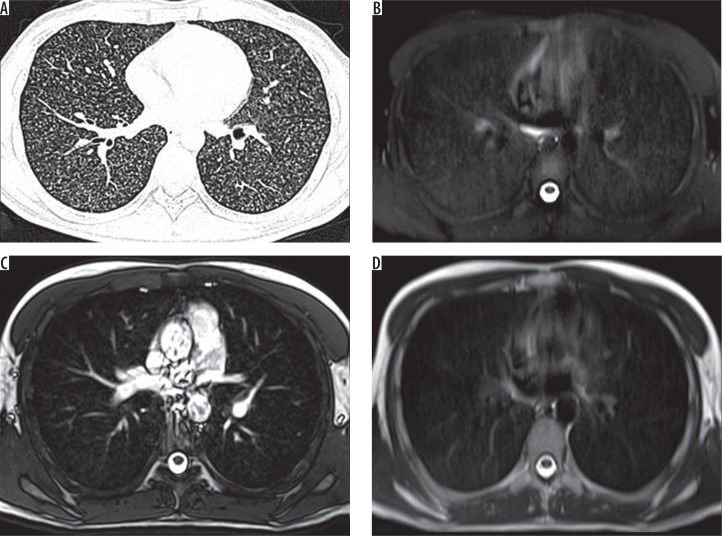
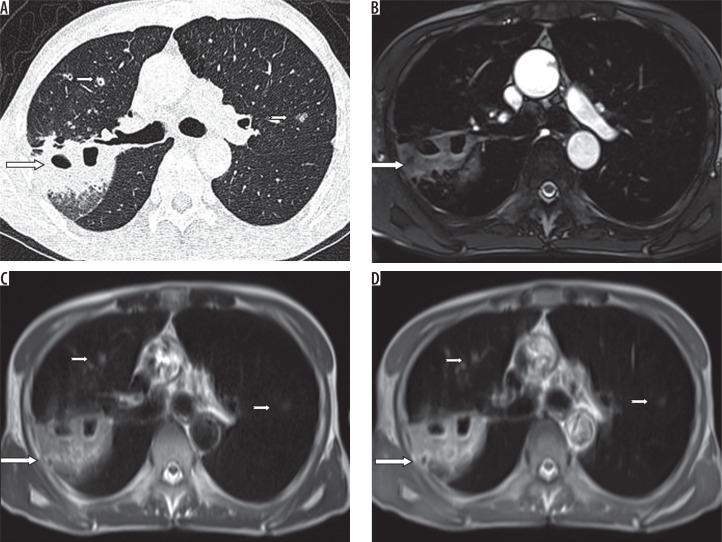
Computed tomography (CT) and MRI chest were performed in 35 immuno-compromised patients suspected of pulmonary infection. The MRI sequences that were performed included axial and coronal T2 half-Fourier acquisition single-shot turbo spin-echo (HASTE), spectrally attenuated inversion recovery (SPAIR), true fast imaging with steady-state free precession (TRUFI), and three-dimensional fast low angle shot (3D FLASH) using breath-hold and respiratory triggered BLADE (proprietary name for periodically rotated overlapping parallel lines with enhanced reconstruction). The presence of nodules, consolidations, and ground-glass opacities was evaluated. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for MRI using CT scan as a reference standard.
The sensitivity of MRI in nodule detection was 50% overall and 75% for nodules measuring more than 5 mm. Consolidation was detected with 100% sensitivity. Sensitivity and PPV for the detection of ground-glass opacities (GGOs) were 77.7% and 53.8%, respectively. T2 HASTE axial had the fewest image artefacts. Respiratory triggered MR pulse sequence did not add any significant diagnostic information as compared to the non-respiratory triggered MR pulse sequences.
Sensitivity for detecting small nodules and GGOs on MR is poor; CT scan remains the imaging modality of choice for the evaluation of pulmonary infections in immunocompromised patients. However, MRI can be used in the follow-up imaging of these patients.
评估磁共振成像(MRI)在诊断免疫功能低下成人肺部感染中的准确性。
对35例疑似肺部感染的免疫功能低下患者进行胸部计算机断层扫描(CT)和MRI检查。所采用的MRI序列包括轴位和冠状位T2加权半傅里叶采集单次激发快速自旋回波(HASTE)序列、频谱衰减反转恢复(SPAIR)序列、稳态自由进动快速成像(TRUFI)序列以及采用屏气和呼吸触发刀锋技术(周期性旋转重叠平行线增强重建的专有名称)的三维快速低角度激发(3D FLASH)序列。评估结节、实变和磨玻璃样混浊的存在情况。以CT扫描作为参考标准,计算MRI的敏感性、特异性、阳性预测值(PPV)和阴性预测值(NPV)。
MRI检测结节的总体敏感性为50%,对于直径大于5mm的结节敏感性为75%。实变的检测敏感性为100%。磨玻璃样混浊(GGOs)检测的敏感性和PPV分别为77.7%和53.8%。T2加权HASTE轴位序列的图像伪影最少。与非呼吸触发的MR脉冲序列相比,呼吸触发的MR脉冲序列未增加任何显著的诊断信息。
MRI检测小结节和GGOs的敏感性较差;CT扫描仍是评估免疫功能低下患者肺部感染的首选成像方式。然而,MRI可用于这些患者的随访成像。