Dahlgren David, Cano-Cebrián Maria-Jose, Olander Tobias, Hedeland Mikael, Sjöblom Markus, Lennernäs Hans
Department of Pharmacy, Division of Biopharmaceutics, Uppsala University, 752 36 Uppsala, Sweden.
Department of Pharmacy and Pharmaceutical Technology and Parasitology, University of Valencia, 46010 València, Spain.
Pharmaceutics. 2020 Mar 8;12(3):242. doi: 10.3390/pharmaceutics12030242.
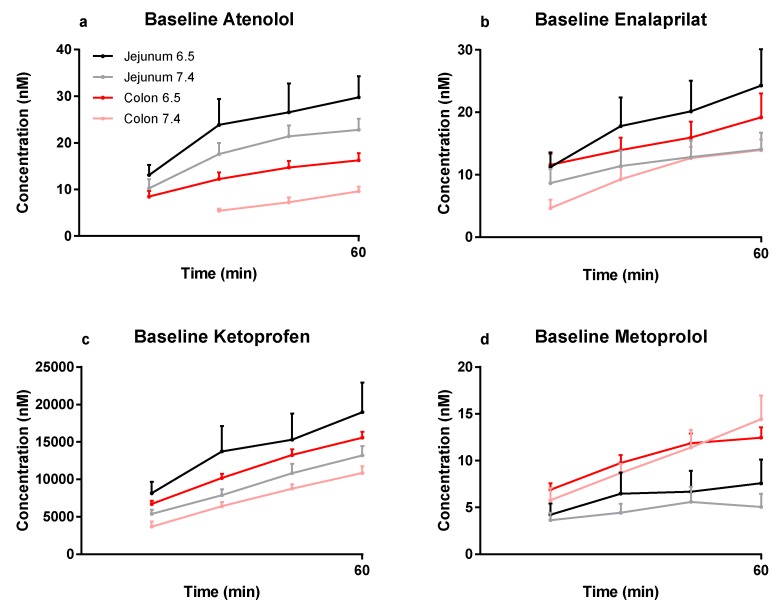
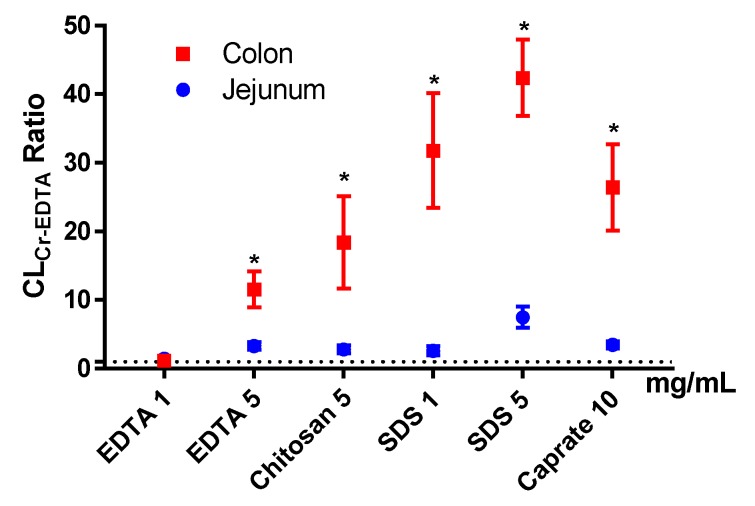
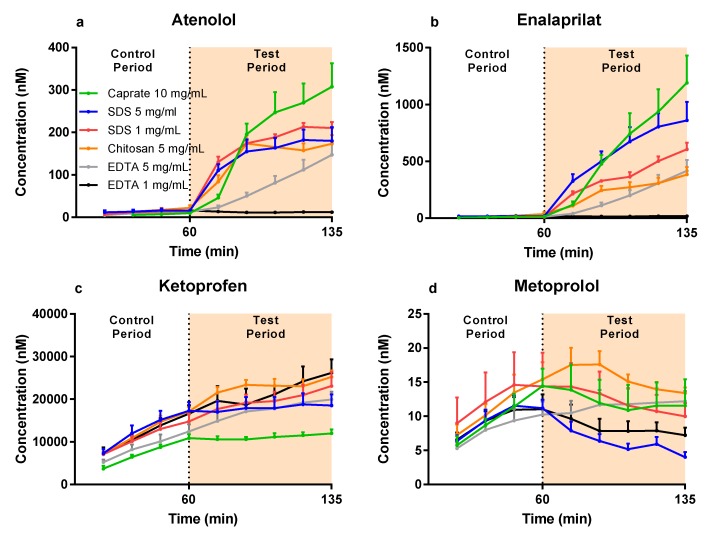
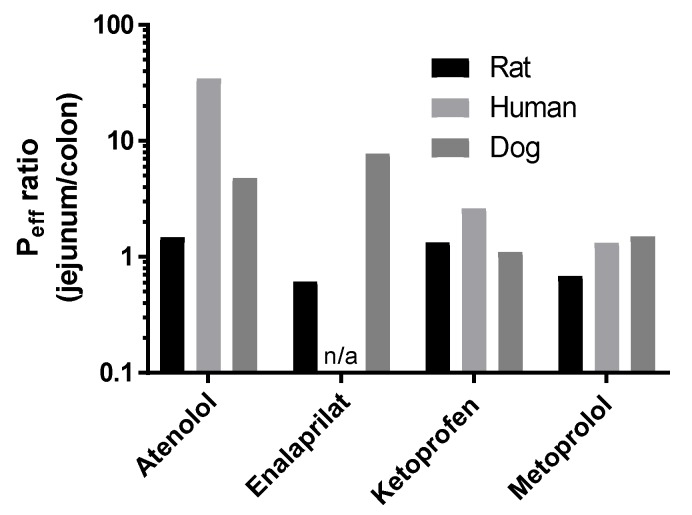
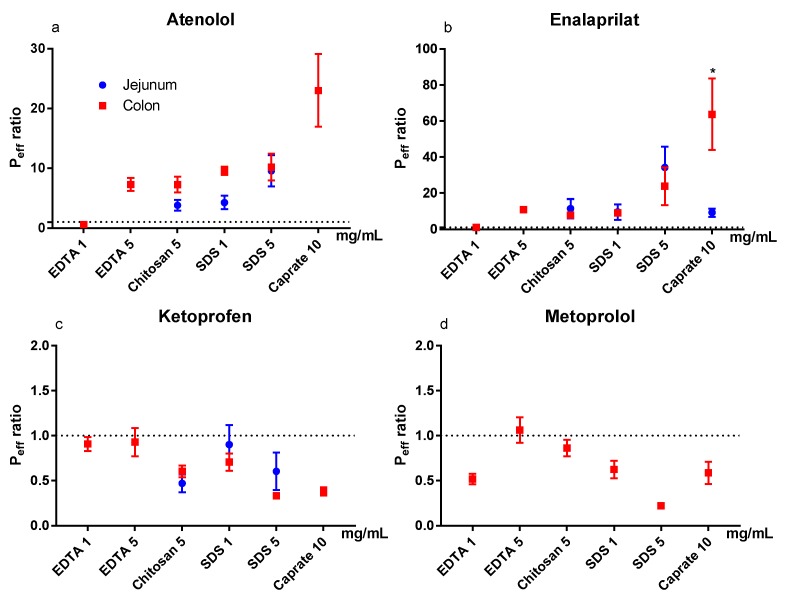
Sufficient colonic absorption is necessary for all systemically acting drugs in dosage forms that release the drug in the large intestine. Preclinically, colonic absorption is often investigated using the rat single-pass intestinal perfusion model. This model can determine intestinal permeability based on luminal drug disappearance, as well as the effect of permeation enhancers on drug permeability. However, it is uncertain how accurate the rat single-pass intestinal perfusion model predicts regional intestinal permeability and absorption in human. There is also a shortage of systematic in vivo investigations of the direct effect of permeation enhancers in the small and large intestine. In this rat single-pass intestinal perfusion study, the jejunal and colonic permeability of two low permeability drugs (atenolol and enalaprilat) and two high-permeability ones (ketoprofen and metoprolol) was determined based on plasma appearance. These values were compared to already available corresponding human data from a study conducted in our lab. The colonic effect of four permeation enhancers-sodium dodecyl sulfate, chitosan, ethylenediaminetetraacetic acid (EDTA), and caprate-on drug permeability and transport of chromium EDTA (an established clinical marker for intestinal barrier integrity) was determined. There was no difference in jejunal and colonic permeability determined from plasma appearance data of any of the four model drugs. This questions the validity of the rat single-pass intestinal perfusion model for predicting human regional intestinal permeability. It was also shown that the effect of permeation enhancers on drug permeability in the colon was similar to previously reported data from the rat jejunum, whereas the transport of chromium EDTA was significantly higher ( < 0.05) in the colon than in jejunum. Therefore, the use of permeation enhancers for increasing colonic drug permeability has greater risks than potential medical rewards, as indicated by the higher permeation of chromium EDTA compared to the drugs.
对于所有在大肠中释放药物的全身作用剂型的药物而言,充分的结肠吸收是必要的。临床前研究中,结肠吸收通常采用大鼠单通道肠灌注模型进行研究。该模型可以根据肠腔药物消失情况确定肠道通透性,以及渗透促进剂对药物通透性的影响。然而,大鼠单通道肠灌注模型预测人体局部肠道通透性和吸收的准确性尚不确定。此外,对于渗透促进剂在小肠和大肠中的直接作用,缺乏系统性的体内研究。在这项大鼠单通道肠灌注研究中,基于血浆出现情况测定了两种低通透性药物(阿替洛尔和依那普利拉)以及两种高通透性药物(酮洛芬和美托洛尔)的空肠和结肠通透性。将这些值与我们实验室进行的一项研究中已有的相应人体数据进行了比较。测定了四种渗透促进剂——十二烷基硫酸钠、壳聚糖、乙二胺四乙酸(EDTA)和癸酸盐——对药物通透性以及铬标记EDTA(一种已确立的肠道屏障完整性临床标志物)转运的结肠效应。根据四种模型药物中任何一种的血浆出现数据所测定的空肠和结肠通透性没有差异。这对大鼠单通道肠灌注模型预测人体局部肠道通透性的有效性提出了质疑。研究还表明,渗透促进剂对结肠中药物通透性的影响与先前报道的大鼠空肠数据相似,而铬标记EDTA在结肠中的转运显著高于空肠(P<0.05)。因此,与潜在的医学益处相比,使用渗透促进剂增加结肠药物通透性的风险更大,这一点从铬标记EDTA比药物具有更高的通透性可以看出。