Department of Pharmacy, Pharmaceutical Technology and Parasitology, University of Valencia, 46100 Burjasot, Spain.
Department of Pharmaceutical Biosciences, Translational Drug Discovery and Development, Uppsala University, 752 36 Uppsala, Sweden.
Int J Mol Sci. 2022 Jan 18;23(3):1021. doi: 10.3390/ijms23031021.
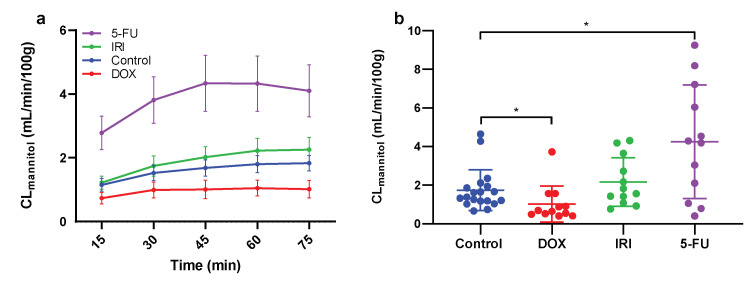
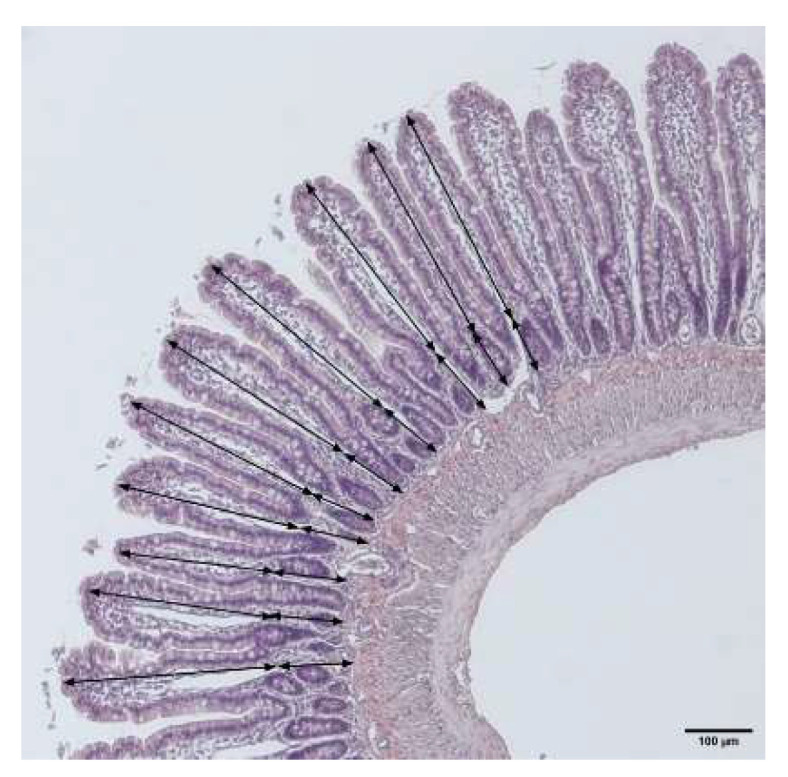
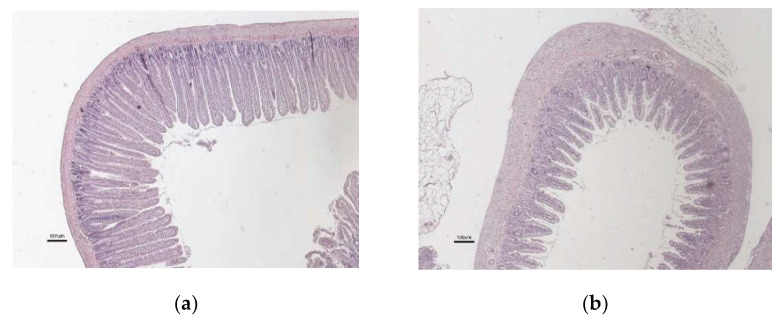
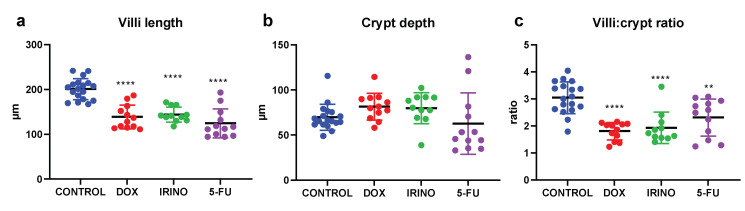
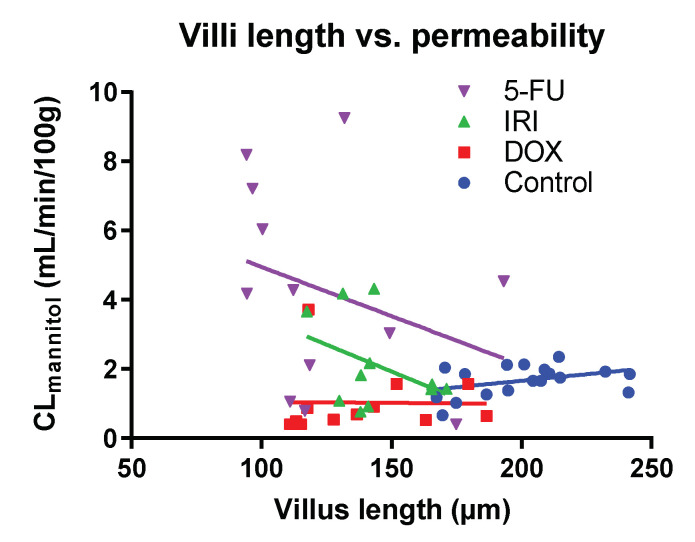
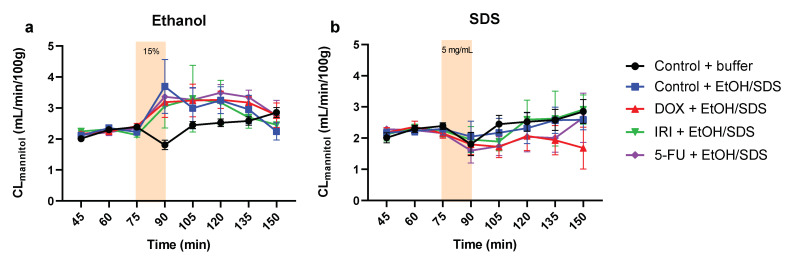
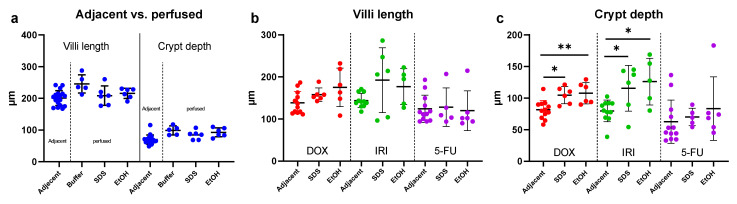
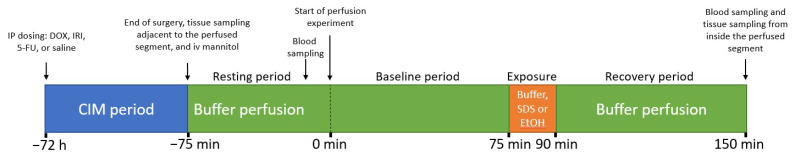
Chemotherapy causes intestinal mucositis, which includes villous atrophy and altered mucosal barrier function. However, there is an uncertainty regarding how the reduced small-intestinal surface area affects the mucosal permeability of the small marker probe mannitol (MW 188), and how the mucosa responds to luminal irritants after chemotherapy. The aims in this study were to determine (i) the relationship between chemotherapy-induced villus atrophy and the intestinal permeability of mannitol and (ii) how the mucosa regulate this permeability in response to luminal ethanol and sodium dodecyl sulfate (SDS). This was investigated by treating rats with a single intraperitoneal dose of doxorubicin, irinotecan, or 5-fluorouracil. After 72 h, jejunum was single-pass perfused and mannitol permeability determined at baseline and after 15 min luminal exposure to 15% ethanol or 5 mg/mL SDS. Tissue samples for morphological analyses were sampled from the perfused segment. All three chemotherapeutics caused a similar 30% reduction in villus length. Mannitol permeability increased with irinotecan (1.3-fold) and 5-fluorouracil (2.5-fold) and was reduced with doxorubicin (0.5-fold), suggesting that it is not epithelial surface area alone that regulates intestinal permeability to mannitol. There was no additional increase in mannitol permeability induced by luminal ethanol or SDS in the chemotherapy-treated rats compared to controls, which may be related to the relatively high basal permeability of mannitol compared to other common low-permeability probes. We therefore suggest that future studies should focus on elucidating the complex interplay between chemotherapy in combination with luminal irritants on the intestinal permeability of other probes.
化疗会导致肠黏膜炎症,包括绒毛萎缩和黏膜屏障功能改变。然而,对于小肠表面积的减少如何影响小分子标志物甘露醇(MW 188)的黏膜通透性,以及化疗后黏膜如何应对腔内容激物,目前还存在不确定性。本研究旨在确定:(i)化疗引起的绒毛萎缩与甘露醇肠黏膜通透性之间的关系;(ii)黏膜如何调节这种通透性以应对腔内容激物乙醇和十二烷基硫酸钠(SDS)。通过给大鼠单次腹腔内注射多柔比星、伊立替康或 5-氟尿嘧啶来实现。72 小时后,对空肠进行单次通过灌注,并在 15%乙醇或 5mg/mL SDS 腔暴露 15 分钟后测定甘露醇通透性。从灌注段取样用于形态学分析的组织样本。三种化疗药物均导致绒毛长度相似地减少 30%。伊立替康(1.3 倍)和 5-氟尿嘧啶(2.5 倍)使甘露醇通透性增加,而多柔比星(0.5 倍)使甘露醇通透性降低,表明调节甘露醇肠黏膜通透性的不仅仅是上皮表面积。与对照组相比,在接受化疗的大鼠中,腔内容激物乙醇或 SDS 并未引起甘露醇通透性的进一步增加,这可能与甘露醇与其他常见低通透性探针相比具有相对较高的基础通透性有关。因此,我们建议未来的研究应集中阐明化疗与腔内容激物联合作用对其他探针的肠道通透性的复杂相互作用。