Department of Nutrition, Exercise and Sports, University of Copenhagen, Copenhagen, Denmark.
Division of Gastroenterology and Nutrition, Children's Research Centre, University Children's Hospital Zurich, Zurich, Switzerland.
Thyroid. 2020 Sep;30(9):1355-1365. doi: 10.1089/thy.2019.0789. Epub 2020 Apr 28.
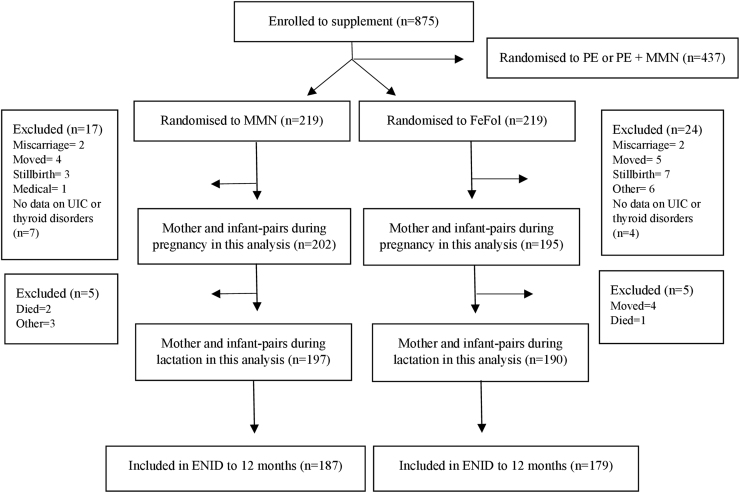
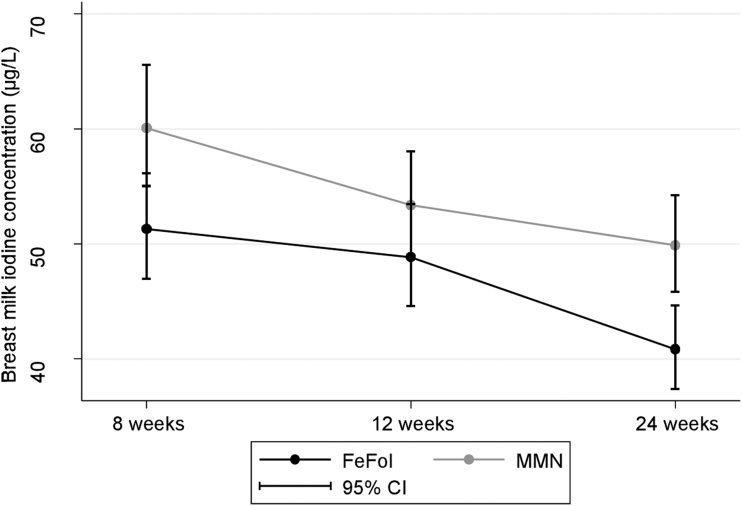
Iodine supplementation is recommended to pregnant women in iodine-deficient populations, but the impact in moderate iodine deficiency is uncertain. We assessed the effect of an iodine-containing prenatal multiple micronutrient (MMN) supplement in a rural Gambian population at risk of moderate iodine deficiency. This study uses data and samples collected as a part of the randomized controlled trial Early Nutrition and Immune Development (ENID; ISRCTN49285450) conducted in Keneba, The Gambia. Pregnant women (<20 weeks gestation) were randomized to either a daily supplement of MMNs containing 300 μg of iodine or an iron and folic acid (FeFol) supplement. Randomization was double blinded (participants and investigators). The coprimary outcomes were maternal urinary iodine concentration (UIC) and serum thyroglobulin (Tg), assessed at baseline and at 30 weeks' gestation. Secondary outcomes were maternal serum thyrotropin (TSH), total triiodothyronine (TT3), total thyroxine (TT4) (assessed at baseline and at 30 weeks' gestation), breast milk iodine concentration (BMIC) (assessed at 8, 12, and 24 weeks postpartum), infant serum Tg (assessed at birth [cord], 12, and 24 weeks postpartum), and serum TSH (assessed at birth [cord]). The effect of supplementation was evaluated using mixed effects models. A total of 875 pregnant women were enrolled between April 2010 and February 2015. In this secondary analysis, we included women from the MMN ( = 219) and FeFol ( = 219) arm of the ENID trial. At baseline, median (interquartile range or IQR) maternal UIC and Tg was 51 μg/L (33-82) and 22 μg/L (12-39), respectively, indicating moderate iodine deficiency. Maternal MMN supplement increased maternal UIC ( < 0.001), decreased maternal Tg ( < 0.001), and cord blood Tg ( < 0.001) compared with FeFol. Maternal thyroid function tests (TSH, TT3, TT4, and TT3/TT4 ratio) and BMIC did not differ according to maternal supplement group over the course of the study. Median (IQR) BMIC, maternal UIC, and infant Tg in the MMN group were 51 μg/L (35-72), 39 μg/L (25-64), and 87 μg/L (59-127), respectively, at 12 weeks postpartum, and did not differ between supplement groups. Supplementing moderately iodine-deficient women during pregnancy improved maternal iodine status and reduced Tg concentration. However, the effects were not attained postpartum and maternal and infant iodine nutrition remained inadequate during the first six months after birth. Consideration should be given to ensuring adequate maternal status through pregnancy and lactation in populations with moderate deficiency.
碘补充剂被推荐给碘缺乏人群中的孕妇,但在中度碘缺乏中的影响尚不确定。我们评估了在有中度碘缺乏风险的冈比亚农村人群中使用含碘的产前多种微量营养素(MMN)补充剂的效果。本研究使用了作为早期营养和免疫发育(ENID;ISRCTN49285450)随机对照试验的一部分在凯内巴收集的数据和样本,该试验在冈比亚进行。孕妇(<20 周妊娠)被随机分配到每日补充 MMN,其中含有 300μg 的碘或补充铁和叶酸(FeFol)。随机分配是双盲的(参与者和研究人员)。主要结局是孕妇尿碘浓度(UIC)和血清甲状腺球蛋白(Tg),在基线和 30 周妊娠时评估。次要结局是孕妇血清促甲状腺激素(TSH)、总三碘甲状腺原氨酸(TT3)、总甲状腺素(TT4)(在基线和 30 周妊娠时评估)、母乳碘浓度(BMIC)(在产后 8、12 和 24 周评估)、婴儿血清 Tg(在出生时[脐带]、产后 12 和 24 周评估)和血清 TSH(在出生时[脐带]评估)。使用混合效应模型评估补充的效果。共有 875 名孕妇于 2010 年 4 月至 2015 年 2 月期间入组。在这项二次分析中,我们纳入了 ENID 试验 MMN(n=219)和 FeFol(n=219)臂的女性。在基线时,中位数(四分位数范围或 IQR)的母体 UIC 和 Tg 分别为 51μg/L(33-82)和 22μg/L(12-39),表明中度碘缺乏。与 FeFol 相比,母体 MMN 补充剂增加了母体 UIC(<0.001),降低了母体 Tg(<0.001)和脐带血 Tg(<0.001)。在研究过程中,母体甲状腺功能测试(TSH、TT3、TT4 和 TT3/TT4 比值)和 BMIC 并未因母体补充剂组而异。在产后 12 周时,MMN 组的中位数(IQR)BMIC、母体 UIC 和婴儿 Tg 分别为 51μg/L(35-72)、39μg/L(25-64)和 87μg/L(59-127),且两组间无差异。
在中度碘缺乏的孕妇怀孕期间补充碘可以改善母体碘状况并降低 Tg 浓度。然而,这些效果并未在产后达到,并且母婴碘营养在出生后六个月内仍然不足。在中度缺乏的人群中,应考虑通过妊娠和哺乳期确保母体充足的状态。