Mansour Sam E, Browning David J, Wong Keye, Flynn Harry W, Bhavsar Abdhish R
George Washington University, Washington, DC, USA.
Virginia Retina Center, Warrenton, VA, 20186, USA.
Clin Ophthalmol. 2020 Mar 4;14:653-678. doi: 10.2147/OPTH.S236637. eCollection 2020.
To review the current therapeutic options for the management of diabetic retinopathy (DR) and diabetic macular edema (DME) and examine the evidence for integration of laser and pharmacotherapy.
A review of the PubMed database was performed using the search terms diabetic retinopathy, diabetic macular edema, neovascularization, laser photocoagulation, intravitreal injection, vascular endothelial growth factor (VEGF), vitrectomy, pars plana vitreous surgery, antiangiogenic therapy. With additional cross-referencing, this yielded 835 publications of which 301 were selected based on content and relevance.
Many recent studies have evaluated the pharmacological, laser and surgical therapeutic strategies for the treatment and prevention of DR and DME. Several newer diagnostic systems such as optical coherence tomography (OCT), microperimetry, and multifocal electroretinography (mfERG) are also assisting in further refinements in the staging and classification of DR and DME. Pharmacological therapies for both DR and DME include both systemic and ocular agents. Systemic agents that promote intensive glycemic control, control of dyslipidemia and antagonists of the renin-angiotensin system demonstrate beneficial effects for both DR and DME. Ocular therapies include anti-VEGF agents, corticosteroids and nonsteroidal anti-inflammatory drugs. Laser therapy, both as panretinal and focal or grid applications continue to be employed in management of DR and DME. Refinements in laser devices have yielded more tissue-sparing (subthreshold) modes in which many of the benefits of conventional continuous wave (CW) lasers can be obtained without the adverse side effects. Recent attempts to lessen the burden of anti-VEGF injections by integrating laser therapy have met with mixed results. Increasingly, vitreoretinal surgical techniques are employed for less advanced stages of DR and DME. The development and use of smaller gauge instrumentation and advanced anesthesia agents have been associated with a trend toward earlier surgical intervention for diabetic retinopathy. Several novel drug delivery strategies are currently being examined with the goal of decreasing the therapeutic burden of monthly intravitreal injections. These fall into one of the five categories: non-biodegradable polymeric drug delivery systems, biodegradable polymeric drug delivery systems, nanoparticle-based drug delivery systems, ocular injection devices and with sustained release refillable devices. At present, there remains no one single strategy for the management of the particular stages of DR and DME as there are many options that have not been rigorously tested through large, randomized, controlled clinical trials.
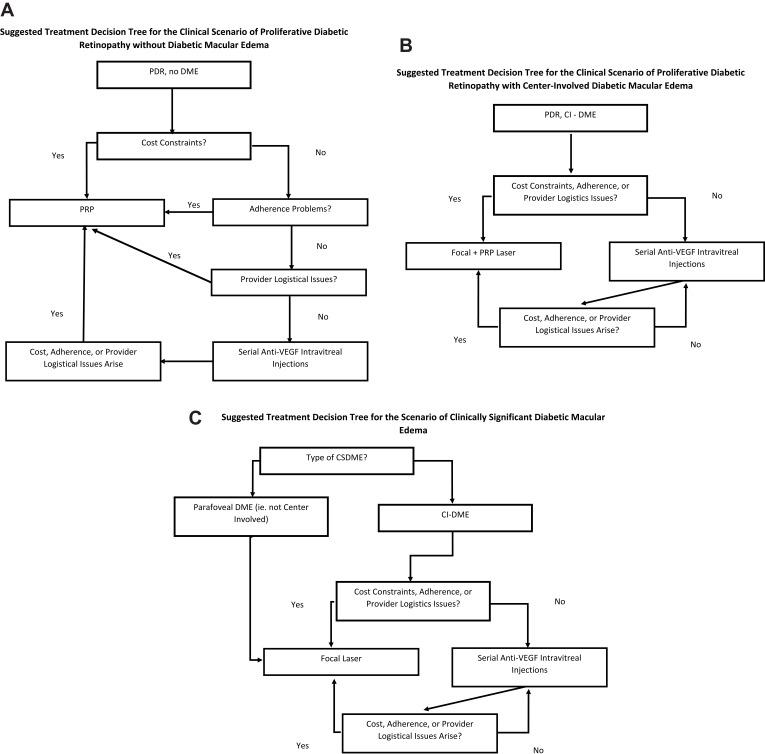
Pharmacotherapy, both ocular and systemic, will be the primary mode of intervention in the management of DR and DME in many cases when cost and treatment burden are less constrained. Conventional laser therapy has become a secondary intervention in these instances, but remains a first-line option when cost and treatment burden are more constrained. Results with subthreshold laser appear promising but will require more rigorous study to establish its role as adjunctive therapy. Evidence to support an optimal integration of the various treatment options is lacking. Central to the widespread adoption of any therapeutic regimen for DR and DME is substantiation of safety, efficacy, and cost-effectiveness by a body of sound clinical trials.
回顾糖尿病视网膜病变(DR)和糖尿病性黄斑水肿(DME)当前的治疗选择,并探讨激光与药物治疗联合应用的证据。
使用搜索词糖尿病视网膜病变、糖尿病性黄斑水肿、新生血管形成、激光光凝、玻璃体内注射、血管内皮生长因子(VEGF)、玻璃体切除术、睫状体平坦部玻璃体手术、抗血管生成治疗对PubMed数据库进行检索。通过额外的交叉引用,共获得835篇出版物,其中基于内容和相关性选择了301篇。
最近许多研究评估了DR和DME治疗及预防的药物、激光和手术治疗策略。一些更新的诊断系统,如光学相干断层扫描(OCT)、微视野计和多焦视网膜电图(mfERG),也有助于进一步完善DR和DME的分期及分类。DR和DME的药物治疗包括全身用药和眼用药物。促进强化血糖控制、控制血脂异常的全身药物以及肾素 - 血管紧张素系统拮抗剂对DR和DME均显示出有益效果。眼用治疗包括抗VEGF药物、皮质类固醇和非甾体抗炎药。激光治疗,无论是全视网膜光凝还是局部或格栅光凝,仍用于DR和DME的治疗。激光设备的改进产生了更多保留组织(阈下)模式,在这种模式下可以获得传统连续波(CW)激光的许多益处而无不良副作用。最近试图通过联合激光治疗减轻抗VEGF注射负担的尝试结果不一。越来越多地,玻璃体视网膜手术技术用于DR和DME较早期阶段。更小口径器械和先进麻醉剂的开发与使用使糖尿病视网膜病变的手术干预有提前的趋势。目前正在研究几种新型药物递送策略,目标是减轻每月玻璃体内注射的治疗负担。这些可分为五类:不可生物降解聚合物药物递送系统、可生物降解聚合物药物递送系统、基于纳米颗粒的药物递送系统、眼用注射装置和可缓释可再填充装置。目前,对于DR和DME特定阶段的管理,尚无单一策略,因为许多选择尚未通过大型随机对照临床试验进行严格测试。
在成本和治疗负担限制较小的许多情况下,眼用和全身药物治疗将是DR和DME管理的主要干预方式。在这些情况下,传统激光治疗已成为次要干预手段,但在成本和治疗负担限制较大时仍是一线选择。阈下激光治疗结果似乎很有前景,但需要更严格的研究来确定其作为辅助治疗的作用。缺乏支持各种治疗选择最佳联合应用的证据。DR和DME任何治疗方案广泛应用的核心是一系列可靠的临床试验证实其安全性、有效性和成本效益。